West China Journal of Stomatology ›› 2025, Vol. 43 ›› Issue (3): 314-324.doi: 10.7518/hxkq.2025.2024427
• Special Review • Previous Articles Next Articles
Cui Yingying1,2( ), Ding Chuanyang1,2(), Peng Chaoran2, Zhang Jianyun2, Cai Xinjia1(), Li Tiejun2()
), Ding Chuanyang1,2(), Peng Chaoran2, Zhang Jianyun2, Cai Xinjia1(), Li Tiejun2()
Received:2024-11-26
Revised:2025-03-20
Online:2025-06-01
Published:2025-06-10
Contact:
Cai Xinjia,Li Tiejun
E-mail:cyy1633488108@163.com;yangfreefei@163.com;caixinjia1994@163.com;litiejun22@vip.sina.com
Supported by:CLC Number:
Cui Yingying, Ding Chuanyang, Peng Chaoran, Zhang Jianyun, Cai Xinjia, Li Tiejun. Progress in clinicopathological diagnosis of oral potentially malignant disorders[J]. West China Journal of Stomatology, 2025, 43(3): 314-324.
Add to citation manager EndNote|Ris|BibTeX
Tab 1
The development of the classification of oral potentially malignant disorders
| 口腔癌前病变和癌前状态(1978) | 口腔潜在恶性病变(2005) | 口腔潜在恶性病变(2021) |
|---|---|---|
| 口腔癌前病变 | 口腔白斑 | 口腔白斑 |
| 口腔白斑 | 口腔红斑 | 增殖性疣状白斑 |
| 口腔红斑 | 倒吸烟相关腭部病损 | 口腔红斑 |
| 倒吸烟相关腭部病损 | 口腔黏膜下纤维性变 | 口腔黏膜下纤维性变 |
| 口腔癌前状态 | 光化性唇炎 | 口腔扁平苔藓 |
| 口腔黏膜下纤维性变 | 扁平苔藓 | 光化性唇炎 |
| 光化性唇炎 | 盘状红斑狼疮 | 倒吸烟相关腭部病损 |
| 扁平苔藓 | 先天性角化异常 | 口腔红斑狼疮 |
| 盘状红斑狼疮 | 大疱性表皮松解症 | 先天性角化异常 |
| 口腔苔藓样病变 | ||
| 口腔移植物抗宿主病 |
Tab 2
The development of the definition of oral leukoplakia
| 时间 | 定义 |
|---|---|
| 1978年 | 一种临床上或病理上不能被诊断为其他任何疾病的白色斑块或斑片 |
| 1983年 | 一种临床上或病理上不能被诊断为其他任何疾病,并且除了使用烟草外,不与任何物理或化学致病因素相关的白色斑块或斑片 |
| 1994年 | 一种临床上或病理上不能被诊断为其他任何疾病的发白斑块或斑片,并且除了使用烟草外,不与任何物理或化学致病因素相关 |
| 2007年 | 一种白色的可疑风险斑块,已排除其他已知不增加癌症风险的疾病或病变 |
| 2015年 | 一种主要为白色的斑块或斑片,临床上或病理上不能被诊断为其他任何疾病,增加了在病变区域或口腔其他部位发生癌症的风险 |
| 2021年 | 一种以白色为主的可疑风险斑块,已排除其他已知不增加癌症风险的疾病或病变 |
Tab 3
Biomarkers of malignant transformation of oral leukoplakia
| 癌变生物标志物 | 功能 | 潜在应用 |
|---|---|---|
| 平足蛋白 | 黏蛋白、特异性淋巴管标志物 | 免疫组织化学检测蛋白表达 |
| p53 | 肿瘤蛋白、细胞周期蛋白调节因子 | 免疫组织化学检测蛋白表达 |
| 基因组不稳定性 | 癌症发生特征之一 | DNA非整倍体、杂合性丧失和拷贝数变异等 |
Tab 4
Diagnostic criteria for histopathological grading of oral epithelial dysplasia
| 分级系统 | 组织结构和细胞形态特征 | 分级标准 |
|---|---|---|
| Smith & Pindborg分级(1969) | 滴状上皮钉突,上皮层次紊乱,错角化,基底细胞增生,细胞间黏附丧失,极性丧失,核深染,基底层和棘细胞层的核质比例增加,细胞和细胞核增大,细胞和细胞核形态异常,核分裂象,核分裂象的层次,异常的核分裂象 | 所有特征被分为“无、轻微和明显”三个等级,其中“无”得分为0,“轻微和明显”得分1到10不等,如果所有特征都非常明显,则授予75分。得分0~10为无异常增生;11~25为轻度异常增生;26~45为中度异常增生;>45为重度异常增生 |
| Ljubljana分级(2003) | 棘细胞层增厚,基底细胞层和副基底细胞层的细胞成分保持不变 | 单纯增生 |
| 基底细胞层和副基底细胞层的增殖扩展至总上皮厚度的一半,包含核中等增大的细胞,偶尔出现有丝分裂(大部分正常),并含有少于5%的错角化细胞 | 异常增生 | |
| 保持明显的上皮细胞分层,许多上皮细胞核显示非典型性(细胞核增大,含有不规则的细胞核形态,染色强度有明显变化),核仁增大、数量增加,核质比例增加,核分裂象增多,频繁出现的错角化细胞 | 非典型性增生 | |
| 上皮分层丧失,细胞改变明显,核分裂象增多及异常核分裂象,扩展至上皮的最顶层 | 原位癌 | |
| Brothwell分级(2003) | 基底层细胞和副基底层细胞增生,核深染,核多形性,滴状上皮钉突 | 0=无异常增生;1=轻度异常增生:基底层和副基底层细胞中核深染和多形性的细胞数量增加;2=中度异常增生:滴状上皮钉突,基底层、副基底层和棘细胞层中核深染和多形性的细胞数量增加;3=重度异常增生:滴状上皮钉突,全部上皮层中核深染和多形性的细胞数量增加;4=原位癌:上皮全层的非典型变化,提示早期浸润,但缺乏实质性证据 |
| WHO(2005) | 组织结构特征:上皮层次紊乱,基底细胞极性丧失,滴状上皮钉突,浅层出现核分裂象,核分裂象增加,基底层以上的细胞出现核分裂象,单个细胞成熟前角化(错角化) 细胞非典型性特征:细胞核增大,细胞核形态异常(核多形性),细胞增大,细胞形态异常(细胞多形性),核质比例增加,异常核分裂象,核仁增大、数量增加 | 1)单纯增生:基底层/副基底层细胞增生,无细胞异型性;2)轻度上皮异常增生:仅限于上皮下1/3的组织结构紊乱,伴有细胞学非典型性;3)中度上皮异常增生:组织结构紊乱延伸至上皮中1/3,细胞非典型性较明显时可诊断为重度异常增生;4)重度上皮异常增生:组织结构紊乱扩展至上皮的2/3以上;5)原位癌:全层或几乎全层的组织结构紊乱,伴有明显的细胞非典型性 |
| 二分类系统(2006) | 同WHO(2005) | 1)高风险病变:至少呈现4种组织结构变化和5种细胞非典型性改变;2)低风险病变:呈现少于4种组织结构变化或少于5种细胞非典型性改变 |
| WHO(2017) | 组织结构特征:上皮层次紊乱,基底细胞极性丧失,滴状上皮钉突,核分裂象增加,浅层出现核分裂象,单个细胞成熟前角化(错角化),基底层以上的细胞出现核分裂象,细胞间黏附丧失 细胞非典型性特征:细胞核增大,核多形性,细胞增大,细胞多形性,核质比例增加,异常核分裂象,核仁增大、数量增加,核深染 | 单纯增生、轻度异常增生、中度异常增生、重度异常增生、原位癌分级标准同WHO(2005) 高/低级别异常增生的二分类法被建议,但使用前需要验证 |
| WHO(2022) | 组织结构特征:上皮层次紊乱,基底细胞极性丧失,滴状上皮钉突,基底细胞聚集/成巢,扩大的增殖区域,浅层出现核分裂象,基底层以上细胞出现核分裂象,非角化层出现角化,广泛的成熟前角化(错角化),细胞黏附性下降,无角化上皮出现角化和角化上皮出现过角化,疣状或乳头状结构,组织结构紊乱沿小腺体导管延伸,具有明显分界的上皮异常增生改变,多种类型上皮异常增生,多灶性或跳跃性病变 细胞非典型性特征:细胞核增大,核多形性,细胞增大,细胞多形性,核分裂象增加,核质比例增加,异常核分裂象,核仁增大、数量增加,单个细胞角化,核深染,凋亡核分裂象 | 单纯增生标准同WHO(2005)。在高等级的病变中,组织结构紊乱和细胞非典型性增加,轻度异常增生的特征是细胞非典型性仅限于基底1/3;中度异常增生的特征是扩展到中间1/3;重度异常增生的特征是扩展到上部1/3 这种方式定义分级过于简化了异常增生的复杂性。局限于基底1/3的细胞非典型性,根据存在的个别特征,可能归类为重度异常增生,特别是当存在滴状上皮钉突、基底细胞紊乱和成巢聚集,以及明显的细胞非典型性时 不建议使用口腔原位癌这一术语,它被归类为重度异常增生 高/低级别异常增生的二分类法被建议,但使用前需要验证 |

Fig 1
Oral leukoplakia HE staining ×100

Tab 5
Histopathological diagnostic criteria for oral submucous fibrosis
| 研究者和时间 | 分期 | 组织病理学特征 |
|---|---|---|
| Pindborg(1966) | 最早期 | 细小的胶原纤维,大量成纤维细胞,小血管扩张充血,明显水肿,有中性粒细胞和嗜酸性粒细胞浸润 |
| 早期 | 较致密的胶原纤维,出现胶原纤维玻璃样变,中等数量成纤维细胞,小血管扩张充血,少量水肿,有嗜酸性粒细胞、淋巴细胞和浆细胞浸润 | |
| 中期 | 致密的胶原纤维,胶原纤维中度玻璃样变,少量成纤维细胞,具有延长的纺锤形核和少量胞浆的纤维细胞,小血管正常或狭窄,血管减少,轻微水肿,有淋巴细胞、浆细胞和少量嗜酸性粒细胞浸润 | |
| 晚期 | 更致密的胶原纤维束,胶原纤维全部玻璃样变,延伸至黏膜下层,替代脂肪或纤维血管组织,小唾液腺炎症和肌肉退行性变,组织纤维化,成纤维细胞缺失,小血管完全闭塞,无水肿,有淋巴细胞和浆细胞浸润 | |
| Utsunomiya(2005) | 早期 | 上皮下结缔组织区域有丰富的淋巴细胞浸润,伴黏液水肿样变化 |
| 中期 | 上皮下炎细胞浸润减少,上皮下层玻璃样变,小血管扩张充血,纤维条索形成,肌层附近颗粒样变 | |
| 晚期 | 上皮下炎细胞浸润几乎消失,玻璃样变向肌层扩展,明显的纤维性变,小血管狭窄,肌纤维出现萎缩和退行性变 | |
| Kumar(2007) | Ⅰ期 | 松散的、粗细不一的胶原纤维 |
| Ⅱ期 | 松散或致密的胶原纤维伴有部分玻璃样变 | |
| Ⅲ期 | 胶原纤维完全玻璃样变 | |
| WHO(2022) | 最初,上皮增生,随后发展为明显萎缩,上皮钉突消失。随着疾病进展可能出现上皮异常增生,钉突肥大是最早期的异常增生特征 | |
| 早期 | 黏膜下层的变化最小,仅有轻微的血管增多、炎细胞浸润,以及胶原原纤维和胶原纤维束的增加,其间散布成纤维细胞 | |
| 中期 | 胶原变得均质化,上皮下方出现胶原纤维玻璃样变 | |
| 晚期 | 血管闭塞,胶原纤维玻璃样变,致密的纤维性变延伸到下层组织,伴有肌肉退行性变和疏松结缔组织(海绵状和网状组织)被纤维组织完全替代 |

Fig 2
Oral submucous fibrosis HE staining

Tab 6
Clinical diagnostic criteria for proliferative verrucous leukoplakia
| 研究者和时间 | 诊断标准 |
|---|---|
| Hansen(1985) | 一种特殊的口腔白斑病,起初表现为单纯的角化过度,但倾向于在不同时间段内扩展并变得多灶性。这些病变生长缓慢、持续存在、不可逆,并且经常发展出红斑成分。一些区域后来变得外生性并呈现疣状,转变成临床上和显微镜下与疣状癌和鳞状细胞癌相同的病变。此外,对各种治疗都具有抗性 |
| Cerero-Lapiedra(2010) | 主要标准:1)具有2个以上不同口腔部位的白斑病变,最常见于牙龈、牙槽突和硬腭;2)存在疣状区域;3)病变在疾病发展过程中有扩散或增大的情况;4)在先前治疗过的区域有复发;5)组织病理学上,可以从简单的上皮角化过度到疣状增生、疣状癌或口腔鳞状细胞癌,无论是原位癌或浸润性癌 |
| 次要标准:1)一个口腔白斑病变,所有受影响区域累计至少占据3 cm;2)患者为女性;3)患者(男性或女性)为非吸烟者;4)疾病发展超过5年 | |
| 增殖性疣状白斑的诊断:3个主要标准,其中必须包括第5个主要标准;或者2个主要标准+2个次要标准,其中必须包括第5个主要标准 | |
| Carrard(2013) | 表现为存在疣状或瘤状突起区域,涉及2个以上的口腔亚部位,包括:舌背(单侧或双侧)、舌缘、颊黏膜、上颌牙槽黏膜或牙龈、下颌牙槽黏膜或牙龈、硬腭、软腭、口底、上唇和下唇;累计所有部位的最小尺寸应至少为3 cm;至少有5年的疾病发展期,且有明确的记录,特征为扩散和增大,以及在先前治疗过的区域发生一次或多次复发;至少有一次活检,以排除疣状癌或鳞状细胞癌的存在 |
| Villa(2018) | 可能是平滑的、有裂纹的、疣状的,伴有或不伴有溃疡的红斑/角化性病变;多灶性非连续性病变或单个部位大病变>4 cm,或影响多个部位中的单个大病变>3 cm;随着时间的推移,病变的大小会进展/扩大和/或发展为多灶性;组织病理学上,如果不明确显示异形增生或癌,显示角化过度、不全角化、萎缩或棘层增生,轻微或无细胞学异型性,伴或不伴淋巴细胞浸润带,或疣状增生;这些特征不得支持摩擦性或反应性角化病的诊断 |
| Lafuente(2021) | 口腔黏膜2个以上不同部位出现多个白斑;出现临床均质和/或非均质白斑(疣状、红白斑、斑点状、结节状);白斑在发展过程中增殖、增长和扩散;以及在先前治疗过的区域出现复发性白斑 |
| 美国口腔颌面部病理学会和北美头颈部病理学家学会(2021) | 将增殖性疣状白斑分为三类病变:非反应性的波纹状过度正角化或不全角化;非反应性的大面积过度角化的上皮增生;疑似鳞状细胞癌或鳞状细胞癌 |

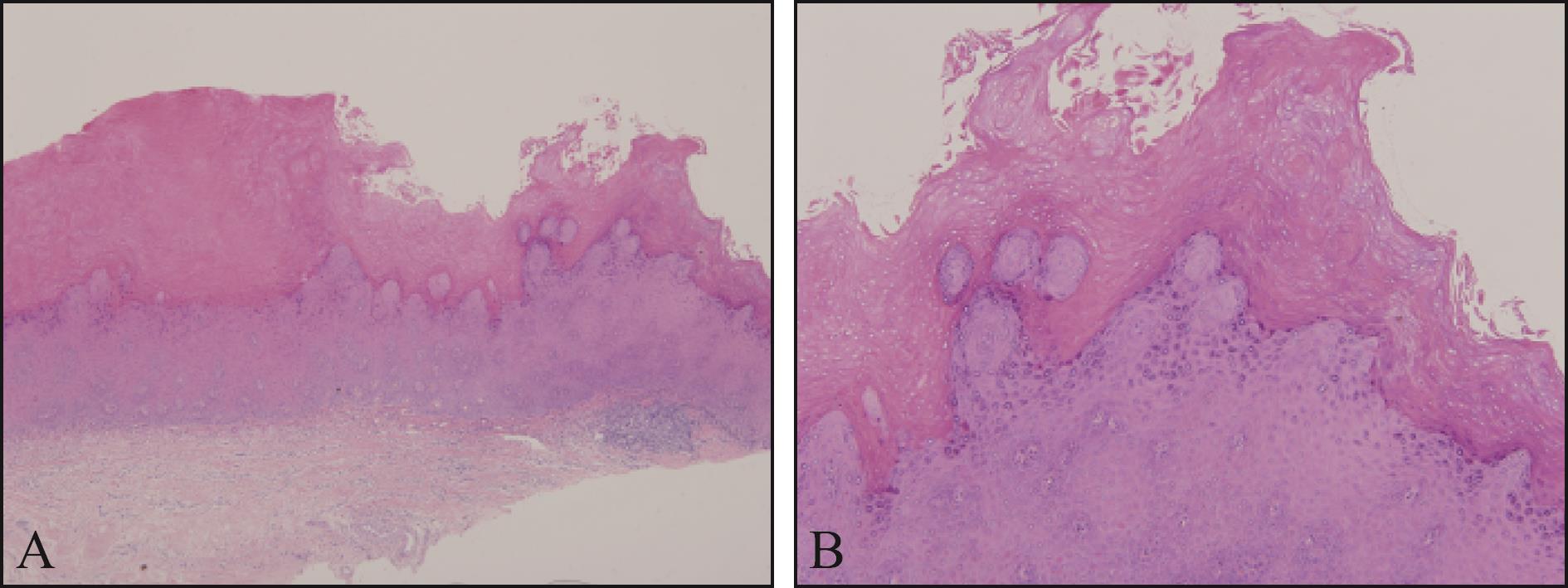
Fig 3
Proliferative verrucous leukoplakia HE staining
Tab 7
Clinical and pathological diagnostic criteria for oral lichen planus
| 研究者和时间 | 诊断标准 |
|---|---|
| van der Meij(2003) | 临床标准:存在双侧、或多或少对称的病变;存在略微凸起的灰白色线状网络(网状型);糜烂、萎缩、结节和斑块型病变只有在口腔黏膜其他部位存在网状病变时才被视为亚型;对于所有类似扁平苔藓但不符合上述标准的其他病变,应使用“临床符合”一词 |
| 组织病理学标准:存在一个局限于结缔组织浅层的界限清楚的淋巴细胞浸润带;基底层“液化变性”;无上皮异常增生;当组织病理学特征不太明显时,应使用“组织病理学符合”一词 | |
| 口腔扁平苔藓的最终诊断:需要同时满足临床和组织病理学标准 | |
| 在以下情况使用“口腔苔藓样病变”一词:临床上典型口腔扁平苔藓,但组织病理学上仅“符合”口腔扁平苔藓;组织病理学上典型口腔扁平苔藓,但临床上仅“符合”口腔扁平苔藓;临床上“符合”口腔扁平苔藓,组织病理学上“符合”口腔扁平苔藓 | |
| Cheng(2016) | 临床标准:多病灶对称分布;呈现以下一种或多种形式的白色和红色病变,网状/丘疹、萎缩(红斑)、糜烂(溃疡)、斑块、大疱;病变不局限于无烟烟草放置的特定部位,病变不局限于紧邻并与牙科修复物接触的部位,病变的起始与药物的使用无关,病变的起始与使用含过敏性的产品无关 |
| 组织病理学标准:固有层中出现带状或斑片状淋巴细胞浸润,局限于上皮与固有层交界处;基底细胞液化变性;淋巴细胞外渗;无上皮异常增生;无疣状上皮结构变化 | |
| González-Moles(2021) | 临床标准:口腔黏膜任何部位出现白色网状病变;病变的双侧性或对称性不作为诊断标准;伴或不伴萎缩、糜烂、大疱、丘疹或斑块样病变 |
| 排除标准或使口腔扁平苔藓诊断可能性降低的标准:病变与牙科修复材料(主要是银汞合金)的密切接触;病变发展与药物摄入的时间关系密切;有器官移植史,特别是骨髓移植;存在皮肤病变或系统性疾病,提示可能是红斑狼疮 | |
| 组织病理学标准:上皮异常增生是否存在和严重程度,并排除癌症;T淋巴细胞带状浸润,上皮基底层空泡变性和凋亡;在非典型病例中,应进行直接免疫荧光检查,以排除红斑狼疮等疾病 | |
| WHO(2021) | 临床标准:存在双侧、或多或少对称的白色病变,影响颊黏膜、舌、唇和/或牙龈;存在白色丘疹样病变和略微凸起的白色线条(网状、环形或线性)构成的花边状网络,伴或不伴糜烂和溃疡;有时表现为剥脱性龈炎 |
| 组织病理学标准:存在一个界限清楚的淋巴细胞浸润带,局限于结缔组织浅层;基底层和/或副基底层有空泡变性伴角质细胞凋亡的表现;在萎缩型中,由于基底细胞破坏导致上皮再生失败,可能会出现上皮变薄,有时伴有溃疡,可能会发现混合性炎症细胞浸润 |
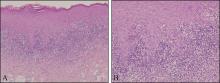
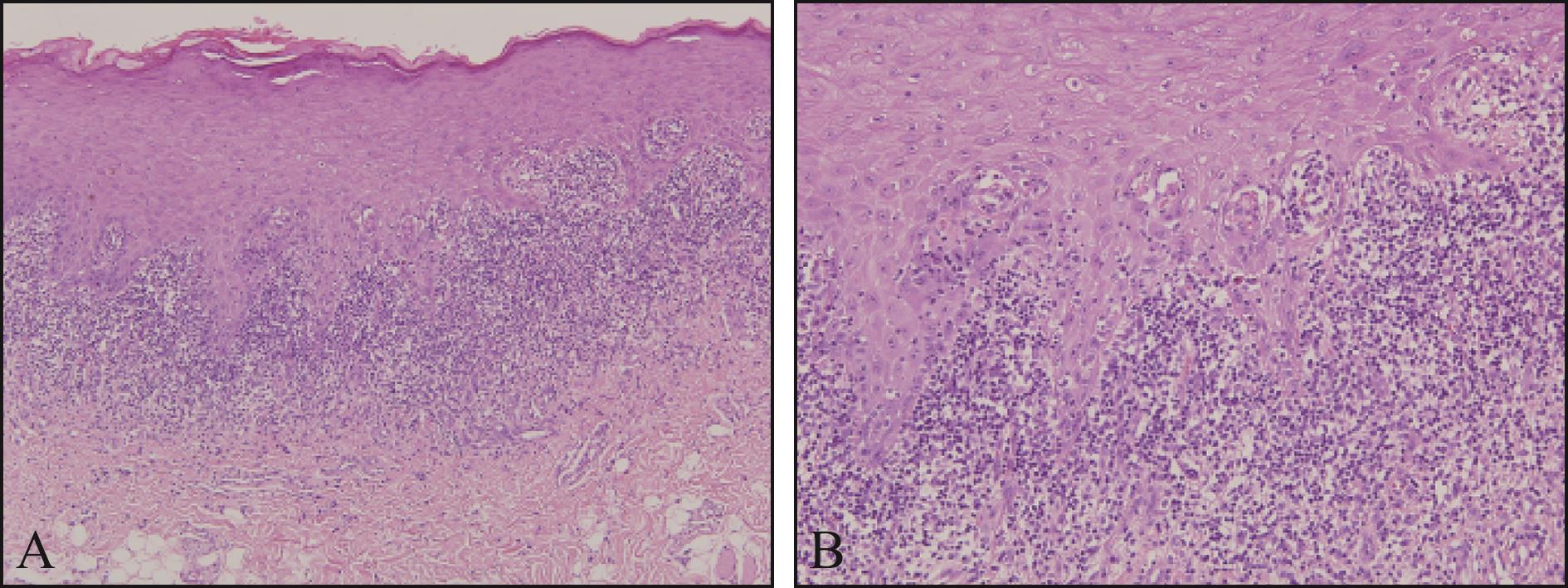
Fig 4
Oral lichen planus HE staining
Tab 8
Biomarkers of malignant transformation of oral potentially malignant disorders
| 生物标志物 | 纳入文献 | 纳入病例 | 癌变风险 | 检测方式 |
|---|---|---|---|---|
| p53 | 1 210 | 相对风险1.88(95%CI:1.39~2.56) | 免疫组织化学 | |
| cyclin D1 | 401 | 风险比2.27(95%CI:1.32~3.91) | 免疫组织化学 | |
| p16 | 496 | 风险比2.01(95%CI:1.36~2.96) | 免疫组织化学 | |
| DNA非整倍体 | 528 | 风险比3.12(95%CI:1.86~5.24) | 细胞DNA图像定量分析 |
| 1 | Kramer IR, Lucas RB, Pindborg JJ, et al. Definition of leukoplakia and related lesions: an aid to studies on oral precancer[J]. Oral Surg Oral Med Oral Pathol, 1978, 46(4): 518-539. |
| 2 | Warnakulasuriya S, Johnson NW, van der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa[J]. J Oral Pathol Med, 2007, 36(10): 575-580. |
| 3 | Warnakulasuriya S, Kujan O, Aguirre-Urizar JM, et al. Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer[J]. Oral Dis, 2021, 27(8): 1862-1880. |
| 4 | Mello FW, Miguel AFP, Dutra KL, et al. Prevalence of oral potentially malignant disorders: a systematic review and meta-analysis[J]. J Oral Pathol Med, 2018, 47(7): 633-640. |
| 5 | Aguirre-Urizar JM, Aguirre-Urizar JM, Lafuente-Ibáñez de Mendoza I, et al. Malignant transformation of oral leukoplakia: systematic review and meta-analysis of the last 5 years[J]. Oral Dis, 2021, 27(8): 1881-1895. |
| 6 | Cai X, Zhang J, Han Y, et al. Development and vali-dation of a nomogram prediction model for malignant transformation of oral potentially malignant disorders[J]. Oral Oncol, 2021, 123: 105619. |
| 7 | Monteiro L, Mello FW, Warnakulasuriya S. Tissue biomarkers for predicting the risk of oral cancer in patients diagnosed with oral leukoplakia: a systematic review[J]. Oral Dis, 2021, 27(8): 1977-1992. |
| 8 | Cai X, Zhang J, Zhang H, et al. Biomarkers of malignant transformation in oral leukoplakia: from bench to bedside[J]. J Zhejiang Univ Sci B, 2023, 24(10): 868-882. |
| 9 | Cai X, Zhang J, Li L, et al. Copy number alterations predict development of OSCC from oral leukoplakia[J]. J Dent Res, 2024, 103(2): 138-146. |
| 10 | Monteiro L, Mariano LC, Warnakulasuriya S. Podoplanin could be a predictive biomarker of the risk of patients with oral leukoplakia to develop oral cancer: a systematic review and meta-analysis[J]. Oral Dis, 2024, 30(2): 207-215. |
| 11 | Villa A, Celentano A, Glurich I, et al. World Workshop on Oral Medicine Ⅶ: prognostic biomarkers in oral leukoplakia: a systematic review of longitudinal studies[J]. Oral Dis, 2019, 25(): 64-78. |
| 12 | Celentano A, Glurich I, Borgnakke WS, et al. World Workshop on Oral Medicine Ⅶ: prognostic biomarkers in oral leukoplakia and proliferative verrucous leukop-lakia—a systematic review of retrospective studies[J]. Oral Dis, 2021, 27(4): 848-880. |
| 13 | Odell EW. Aneuploidy and loss of heterozygosity as risk markers for malignant transformation in oral mucosa[J]. Oral Dis, 2021, 27(8): 1993-2007. |
| 14 | Ramos-García P, González-Moles MÁ, Warnakulasuriya S. Significance of p53 overexpression in the prediction of the malignant transformation risk of oral potentially malignant disorders: a systematic review and meta-analysis[J]. Oral Oncol, 2022, 126: 105734. |
| 15 | Odell E, Kujan O, Warnakulasuriya S, et al. Oral epithelial dysplasia: recognition, grading and clinical significance[J]. Oral Dis, 2021, 27(8): 1947-1976. |
| 16 | Tilakaratne WM, Jayasooriya PR, Jayasuriya NS, et al. Oral epithelial dysplasia: causes, quantification, prognosis, and management challenges[J]. Periodontol 2000, 2019, 80(1): 126-147. |
| 17 | Hellquist H, Cardesa A, Gale N, et al. Criteria for grading in the Ljubljana classification of epithelial hyperplastic laryngeal lesions. A study by members of the Working Group on Epithelial Hyperplastic Laryngeal Lesions of the European Society of Pathology[J]. Histopathology, 1999, 34(3): 226-233. |
| 18 | Brothwell DJ, Lewis DW, Bradley G, et al. Observer agreement in the grading of oral epithelial dysplasia[J]. Community Dent Oral Epidemiol, 2003, 31(4): 300-305. |
| 19 | Kujan O, Oliver RJ, Khattab A, et al. Evaluation of a new binary system of grading oral epithelial dysplasia for prediction of malignant transformation[J]. Oral Oncol, 2006, 42(10): 987-993. |
| 20 | Cai X, Zhang J, Zhang H, et al. Architectural and cytological features of epithelial dysplasia associated with transformation risk[J]. Oral Dis, 2024, 30(5): 3028-3038. |
| 21 | Arsenic R, Kurrer MO. Differentiated dysplasia is a frequent precursor or associated lesion in invasive squamous cell carcinoma of the oral cavity and pharynx[J]. Virchows Arch, 2013, 462(6): 609-617. |
| 22 | Becker AS, Holm M, Liese J, Engel N, Zimpfer AH. Diagnosis of differentiated dysplasia as a variant of oral epithelial dysplasia[J]. Oral Dis, 2024, 30(7): 4185-4194. |
| 23 | Wils LJ, Poell JB, LANPeferoen, et al. The role of differentiated dysplasia in the prediction of malignant transformation of oral leukoplakia[J]. J Oral Pathol Med, 2023, 52(10): 930-938. |
| 24 | Brouns ER, Evren I, Wils LJ, et al. Oral leukoplakia classification and staging system with incorporation of differentiated dysplasia[J]. Oral Dis, 2023, 29(7): 2667-2676. |
| 25 | Wils LJ, Poell JB, Evren I, et al. Incorporation of differentiated dysplasia improves prediction of oral leukoplakia at increased risk of malignant progression[J]. Mod Pathol, 2020, 33(6): 1033-1040. |
| 26 | de la Cour CD, Sperling CD, Belmonte F, et al. Prevalence of human papillomavirus in oral epithelial dysplasia: systematic review and meta-analysis[J]. Head Neck, 2020, 42(10): 2975-2984. |
| 27 | Cai X, Yao Z, Liu G, et al. Oral submucous fibrosis: a clinicopathological study of 674 cases in China[J]. J Oral Pathol Med, 2019, 48(4): 321-325. |
| 28 | Kujan O, Mello FW, Warnakulasuriya S. Malignant transformation of oral submucous fibrosis: a systematic review and meta-analysis[J]. Oral Dis, 2021, 27(8): 1936-1946. |
| 29 | Ray JG, Ranganathan K, Chattopadhyay A. Malignant transformation of oral submucous fibrosis: overview of histopathological aspects[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2016, 122(2): 200-209. |
| 30 | Gupta S, Subbappa A, Singh S, et al. Challenges in the classification of oral submucous fibrosis and proposing a new classification based on systematic review of literature[J]. J Int Soc Prev Community Dent, 2023, 13(1): 17-31.. |
| 31 | Kavitha L, Ranganathan K, Shyam S, et al. Immunohistochemical biomarkers in oral submucous fibrosis: a scoping review[J]. J Oral Pathol Med, 2022, 51(7): 594-602. |
| 32 | Hansen LS, Olson JA, Silverman S Jr. Proliferative verrucous leukoplakia. A long-term study of thirty patients[J]. Oral Surg Oral Med Oral Pathol, 1985, 60(3): 285-298. |
| 33 | Ramos-García P, González-Moles MÁ, Mello FW, et al. Malignant transformation of oral proliferative verrucous leukoplakia: a systematic review and meta-analysis[J]. Oral Dis, 2021, 27(8): 1896-1907. |
| 34 | Palaia G, Bellisario A, Pampena R, et al. Oral proliferative verrucous leukoplakia: progression to malignancy and clinical implications. Systematic review and Meta-analysis[J]. Cancers (Basel), 2021, 13(16): 4085. |
| 35 | Lafuente Ibáñez de Mendoza I, Lorenzo Pouso AI, Aguirre Urízar JM, et al. Malignant development of proliferative verrucous/multifocal leukoplakia: a critical systematic review, meta-analysis and proposal of diagnostic criteria[J]. J Oral Pathol Med, 2022, 51(1): 30-38. |
| 36 | Proaño-Haro A, Bagan L, Bagan JV. Recurrences following treatment of proliferative verrucous leukoplakia: a systematic review and meta-analysis[J]. J Oral Pathol Med, 2021, 50(8): 820-828. |
| 37 | Faustino ISP, de Pauli Paglioni M, de Almeida Mariz BAL, et al. Prognostic outcomes of oral squamous cell carcinoma derived from proliferative verrucous leukoplakia: a systematic review[J]. Oral Dis, 2023, 29(4): 1416-1431. |
| 38 | González-Moles MÁ, Warnakulasuriya S, Ramos-García P. Prognosis parameters of oral carcinomas developed in proliferative verrucous leukoplakia: a systematic review and meta-analysis[J]. Cancers (Basel), 2021, 13(19): 4843. |
| 39 | McParland H, Warnakulasuriya S. Lichenoid morpho-logy could be an early feature of oral proliferative verrucous leukoplakia[J]. J Oral Pathol Med, 2021, 50(2): 229-235. |
| 40 | Cai X, Zhang J, Zhang H, et al. Overestimated risk of transformation in oral lichen planus[J]. Oral Oncol, 2022, 133: 106025. |
| 41 | González-Moles MÁ, Ramos-García P, Warnakulasuriya S. A scoping review on gaps in the diagnostic criteria for proliferative verrucous leukoplakia: a conceptual propo-sal and diagnostic evidence-based criteria[J]. Cancers (Basel), 2021, 13(15): 3669. |
| 42 | Cerero-Lapiedra R, Baladé-Martínez D, Moreno-López LA, et al. Proliferative verrucous leukoplakia: a propo-sal for diagnostic criteria[J]. Med Oral Patol Oral Cir Bucal, 2010, 15(6): e839-e845. |
| 43 | Carrard VC, Brouns ER, van der Waal I. Proliferative verrucous leukoplakia; a critical appraisal of the diagnostic criteria[J]. Med Oral Patol Oral Cir Bucal, 2013, 18(3): e411-e4113. |
| 44 | Villa A, Menon RS, Kerr AR, et al. Proliferative leukoplakia: proposed new clinical diagnostic criteria[J]. Oral Dis, 2018, 24(5): 749-760. |
| 45 | Thompson LDR, Fitzpatrick SG, Müller S, et al. Proliferative verrucous leukoplakia: an expert consensus gui-deline for standardized assessment and reporting[J]. Head Neck Pathol, 2021, 15(2): 572-587. |
| 46 | Ramos-García P, González-Moles MÁ, Warnakulasuriya S. Oral cancer development in lichen planus and related conditions-3.0 evidence level: a systematic review of systematic reviews[J]. Oral Dis, 2021, 27(8): 1919-1935. |
| 47 | González-Moles MÁ, Ramos-García P. Oral lichen planus and related lesions. What should we accept based on the available evidence?[J] Oral Dis, 2023, 29(7): 2624-2637. |
| 48 | Idrees M, Kujan O, Shearston K, et al. Oral lichen planus has a very low malignant transformation rate: a systematic review and meta-analysis using strict diagnostic and inclusion criteria[J]. J Oral Pathol Med, 2021, 50(3): 287-298. |
| 49 | González-Moles MÁ, Warnakulasuriya S, González-Ruiz I, et al. Dysplasia in oral lichen planus: relevance, controversies and challenges. A position paper[J]. Med Oral Patol Oral Cir Bucal, 2021, 26(4): e541-e548. |
| 50 | Rock LD, Laronde DM, Lin I, et al. Dysplasia should not be ignored in lichenoid mucositis[J]. J Dent Res, 2018, 97(7): 767-772. |
| 51 | van der Meij EH, van der Waal I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications[J]. J Oral Pathol Med, 2003, 32(9): 507-512. |
| 52 | Cheng YS, Gould A, Kurago Z, et al. Diagnosis of oral lichen planus: a position paper of the American Academy of Oral and Maxillofacial Pathology[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2016, 122(3): 332-354. |
| 53 | González-Moles MÁ, Ramos-García P, Warnakulasuriya S. An appraisal of highest quality studies reporting malignant transformation of oral lichen planus based on a systematic review[J]. Oral Dis, 2021, 27(8): 1908-1918. |
| 54 | Lorenzo-Pouso AI, Caponio VCA, Vieira E Silva FF, et al. Predictive value of CDKN2A/p16INK4a expression in the malignant transformation of oral potentially malignant disorders: systematic review and meta-analysis[J]. Pathol Res Pract, 2023, 248: 154656. |
| 55 | Alaizari NA, Sperandio M, Odell EW, et al. Meta-analysis of the predictive value of DNA aneuploidy in malignant transformation of oral potentially malignant disorders[J]. J Oral Pathol Med, 2018, 47(2): 97-103. |
| 56 | Ramos-García P, González-Moles MÁ, Ayén Á, et al. Predictive value of CCND1/cyclin D1 alterations in the malignant transformation of potentially malignant head and neck disorders: systematic review and meta-analysis[J]. Head Neck, 2019, 41(9): 3395-3407. |
| [1] | Xie Diya, Shan Danni, Zhang Lei, Chen Sheng, Na Yingyu, Wang Zhiyong. Differences in near-infrared fluorescence imaging and histological analysis of cheek mucosa in golden hamsters with different pathological states [J]. West China Journal of Stomatology, 2024, 42(6): 716-722. |
| [2] | Song Ziyi, Yang Chao, Zhang Yunlong, Zhang Zhujiang, Ren Tianjiao, Zhang Xinyue, Li Xue. Mechanism of mangiferin in the treatment of oral submucous fibrosis based on Gene Expression Omnibus database chip mining combined with network pharmacology and molecular docking [J]. West China Journal of Stomatology, 2024, 42(4): 444-451. |
| [3] | Jia Tingting, Zhang Da, Qi Xiangmin, Wang Caijiao, Yan Shiguo. Oral verrucous xanthoma with oral lichen planus: a case report [J]. West China Journal of Stomatology, 2023, 41(1): 104-109. |
| [4] | Tang Nan, Zhang Yuyao, Cheng Juehua, Zhao Zhibai, Fan Yuan. Cross-talk between CXC chemokine ligand 10-CXC chemokine receptor 3 axis and CC chemokine ligand 17-CC chemokine receptor 4 axis in the pathogenesis of oral lichen planus [J]. West China Journal of Stomatology, 2021, 39(4): 405-412. |
| [5] | Wan Zixin, Zheng Zhijian, Huang Meichang, Chen Yu, Yao Lihong. Expression of Ki-67, Cyclin D1, P53, and P16 in patients with oral leukoplakia and leukoplakia cancerization with spicy diet in Chengdu [J]. West China Journal of Stomatology, 2021, 39(4): 434-440. |
| [6] | Guo Jincai, Xie Hui, Wu Hao, Tong Tiejun. Efficacy of curcumin in the treatment of oral submucous fibrosis: a Meta-analysis [J]. West China Journal of Stomatology, 2021, 39(2): 195-202. |
| [7] | Shi Linjun, Yang Xi, Wu Suning, Liu Wei. Transcriptome array screening and verification of oral leukoplakia carcinogenesis-related hypoxia-responsive gene and microRNA [J]. West China Journal of Stomatology, 2021, 39(1): 20-25. |
| [8] | Pan Yingxiao, Guo Dawei, Li Xin, Liu Hengyi, Lu Shulai. Gene polymorphism in oral lichen planus [J]. West China Journal of Stomatology, 2020, 38(6): 681-686. |
| [9] | Zhang Lingyan, Wang Rong, Liu Ting, Cai Yang. The expression and significance of interleukin-35 receptor in oral lichen planus [J]. West China Journal of Stomatology, 2020, 38(5): 513-518. |
| [10] | Xu Zhi,Lü Fengyuan,Jiang Erhui,Zhao Xiaoping,Shang Zhengjun. Relationship among areca nut, intracellular reactive oxygen species, and autophagy [J]. West China Journal of Stomatology, 2020, 38(1): 80-85. |
| [11] | Bo Yang,Mengfan Fu,Zhangui Tang. Rat model with oral submucous fibrosis induced by arecoline and mechanical stimulation [J]. West China Journal of Stomatology, 2019, 37(3): 260-264. |
| [12] | Peiru Jia, Yunying Huang, Ying Wang, Yang Cai. Correlations between the T helper cell 17/regulatory T cells balance in peripheral blood of patients with oral lichen planus and clinical characteristics [J]. West China Journal of Stomatology, 2018, 36(4): 384-388. |
| [13] | Huang Yunying, Zhou Su, Cai Yang.. Expression of interleukin-12 and interleukin-27 proteins and immune status in serum of patients with oral lichen planus [J]. West China Journal of Stomatology, 2016, 34(2): 140-144. |
| [14] | Zhang Jing, Li Zhen, Wang Jingjiao, Qi Ming.. Expression and significance of retinoid-related orphan receptor γt and 4-1BB/4-1BBL in oral lichen planus [J]. West China Journal of Stomatology, 2013, 31(4): 408-411. |
| [15] | Zuo Wenxin, Li Xiaoyu, Chen Yanqing, Peng Hong. Oral health-related quality of life in patients with oral lichen planus [J]. West China Journal of Stomatology, 2012, 30(1): 40-44. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 This work is licensed under a Creative Commons Attribution 3.0 License.
This work is licensed under a Creative Commons Attribution 3.0 License.
