华西口腔医学杂志 ›› 2025, Vol. 43 ›› Issue (6): 845-859.doi: 10.7518/hxkq.2025.2025078
• 临床研究 • 上一篇
张彦表1( ), 魏美荣2, 赵雪娟2, 齐小蕾3, 左姗姗3, 毛淑梅4, 王军1(), 丁刚1()
), 魏美荣2, 赵雪娟2, 齐小蕾3, 左姗姗3, 毛淑梅4, 王军1(), 丁刚1()
收稿日期:2025-03-01
修回日期:2025-07-03
出版日期:2025-12-01
发布日期:2025-11-27
通讯作者:
王军,丁刚
E-mail:zhangyb@sdsmu.edu.cn;wangjun28@sdsmu.edu.cn;dinggang@sdsmu.edu.cn
作者简介:张彦表,硕士,E-mail:基金资助:
Zhang Yanbiao1(), Wei Meirong2, Zhao Xuejuan2, Qi Xiaolei3, Zuo Shanshan3, Mao Shumei4, Wang Jun1(), Ding Gang1()
Received:2025-03-01
Revised:2025-07-03
Online:2025-12-01
Published:2025-11-27
Contact:
Wang Jun,Ding Gang
E-mail:zhangyb@sdsmu.edu.cn;wangjun28@sdsmu.edu.cn;dinggang@sdsmu.edu.cn
Supported by:摘要:
目的 探讨血浆磷酸化tau217(p-tau217)在牙周炎与轻度认知功能障碍(MCI)间的中介效应。 方法 病例对照研究设计,选取2023年11月—2024年5月在山东第二医科大学第一附属医院神经内科确诊为MCI的患者为病例组(MCI组),以同期在体检中心招募的年龄及受教育水平相匹配的认知功能正常(CN)的志愿者为对照组(CN组)。收集研究参与者的一般人口学资料。采用北京版蒙特利尔认知评估量表(MoCA)、临床痴呆评定量表(CDR)和日常生活能力评估量表(ADL)评估神经心理学功能。完成临床牙周检查,计算牙周感染表面积(PISA),以2018年分类法进行牙周炎分期。抽取晨起空腹肘静脉血,检测血液生化指标,酶联免疫吸附试验(ELISA)检测血浆p-tau217水平。采用独立样本t检验、Mann-Whitney U检验、χ2检验、偏相关分析、多因素Logistic回归分析、多元线性回归分析、限制性立方样条(RCS)回归分析、中介效应分析进行统计学分析。 结果 研究共纳入192例参与者,MCI组和CN组各96例,均完成所有试验检查项目。MCI组牙周炎患病率(63.5%)显著高于CN组(43.8%)(χ2=7.561,P=0.006)。MCI组血浆p-tau217水平[7.00(4.27-9.65)ng/mL]显著高于CN组[2.02(0.80-3.81)ng/mL](Z=-8.108,P<0.001)。偏相关分析显示,血浆p-tau217与各临床牙周指标均呈正相关(均P<0.001)。校正基线协变量后,多因素Logistic回归分析显示,牙周炎是MCI的独立危险因素,牙周炎患者的MCI患病风险是非牙周炎的1.977倍(OR=1.977,95%CI:1.088~3.594,P=0.025);Ⅰ/Ⅱ期牙周炎、Ⅲ/Ⅳ期牙周炎的MCI患病风险分别是非牙周炎的1.878倍(OR=1.878,95%CI:1.029~3.425,P=0.040)和2.625倍(OR=2.625,95%CI:1.073~6.246,P=0.035)。趋势检验显示,MCI患病风险随牙周炎分期数增大而增加(Ptrend=0.016)。校正基线协变量后,多元线性回归分析显示,牙周炎是血浆p-tau217水平升高的独立危险因素(β=3.309,95%CI:2.363~4.254,P<0.001);与非牙周炎相比,Ⅰ/Ⅱ期牙周炎(β=1.838,95%CI:0.869~2.806,P<0.001)和Ⅲ/Ⅳ期牙周炎(β=5.539,95%CI:4.442~6.636,P<0.001)的血浆p-tau217水平均升高。趋势检验显示,血浆p-tau217水平随牙周炎分期数增大而升高(Ptrend<0.001)。RCS分析显示,校正基线协变量后,PISA与MIC患病风险(Poverall =0.002,Pnonlinear=0.344)及血浆p-tau217水平(Poverall<0.001,Pnonlinear=0.140)均呈正向线性剂量-反应关系。校正基线协变量后,中介效应分析显示,血浆p-tau217在牙周炎与MCI关联中存在中介效应,中介占比为13.99%(95% Bootstrap CI:0.38%~49.39%,P=0.038)。 结论 牙周炎是MCI患病风险增加和血浆p-tau217水平升高的危险因素,血浆p-tau217负荷加重在牙周炎与MCI患病风险增加的关联中起中介效应。
张彦表, 魏美荣, 赵雪娟, 齐小蕾, 左姗姗, 毛淑梅, 王军, 丁刚. 血浆磷酸化tau217在牙周炎与轻度认知功能障碍间的中介效应[J]. 华西口腔医学杂志, 2025, 43(6): 845-859.
Zhang Yanbiao, Wei Meirong, Zhao Xuejuan, Qi Xiaolei, Zuo Shanshan, Mao Shumei, Wang Jun, Ding Gang. Mediation analysis of plasma phosphorylated tau217 in the association between periodontitis and mild cognitive impairment[J]. West China Journal of Stomatology, 2025, 43(6): 845-859.
表 1
MCI组和CN组基线特征的比较
| 项目 | MCI组(n=96) | CN组(n=96) | χ2/t/Z值 | P值 |
|---|---|---|---|---|
| 一般资料 | ||||
| 性别 | 0.534a | 0.465 | ||
| 女 | 43(44.8%) | 38(39.6%) | ||
| 男 | 53(55.2%) | 58(60.4%) | ||
| 年龄*/岁 | 55(52-58) | 54(52-60) | -0.898c | 0.369 |
| 受教育水平*/年 | 10(8-12) | 9(8-12) | -1.641a | 0.101 |
| 吸烟 | 24(25.0%) | 13(13.5%) | 4.051a | 0.044 |
| 饮酒 | 29(30.2%) | 22(22.9%) | 1.308a | 0.253 |
| 体育锻炼 | 37(38.5%) | 59(61.5%) | 10.083a | 0.001 |
| 高血压 | 30(31.3%) | 17(17.7%) | 4.761a | 0.029 |
| BMI/(kg/m2) | 23.27±3.75 | 22.06±4.21 | 2.105b | 0.037 |
| 收缩压*/mmHg | 129(123-140) | 129(124-136) | -0.603c | 0.546 |
| 舒张压*/mmHg | 83(81-86) | 83(80-86) | -0.853c | 0.394 |
| 血液检验 | ||||
| GHbA1c*/% | 5.3(5.2-5.7) | 5.2(5.1-5.4) | -2.514c | 0.012 |
| 空腹血糖*/(mol/mL) | 5.5(4.9-6.1) | 5.3(4.8-5.6) | -2.917c | 0.004 |
| 总胆固醇*/(mol/mL) | 4.5(4.2-5.1) | 4.6(4.2-5.0) | -0.269c | 0.788 |
| 甘油三酯/(mol/mL) | 1.16±0.50 | 1.17±0.52 | 0.136b | 0.892 |
| HDL-C*/(mol/mL) | 1.3(1.2-1.5) | 1.4(1.1-1.5) | -0.251c | 0.802 |
| LDL-C*/(mol/mL) | 3.0(2.7-3.4) | 2.8(2.2-3.1) | -3.008c | 0.003 |
| 肌酐*/(mol/mL) | 86(82-91) | 87(82-92) | -0.844c | 0.399 |
| eGFR*/[mL/min/(1.73 m2)] | 104(97-110) | 107(99-112) | -1.285c | 0.199 |
| 神经心理学评估 | ||||
| MoCA*/分 | 22(20-24) | 29(28-30) | -11.743c | <0.001 |
| ADL*/分 | 19(17-21) | 15(14-15) | -12.195c | <0.001 |
| CDR/分 | 0.5 | 0 | - | - |
| 牙周炎 | 61(63.5%) | 42(43.8%) | 7.561a | 0.006 |
| 牙周炎分期 | -3.054c | 0.002 | ||
| Ⅰ期 | 11(11.5%) | 12(12.5%) | ||
| Ⅱ期 | 24(25.0%) | 15(15.6%) | ||
| Ⅲ期 | 17(17.7%) | 9(9.4%) | ||
| Ⅳ期 | 9(9.4%) | 6(6.3%) | ||
| 临床牙周指标* | ||||
| PD/mm | 3.31(2.47-3.79) | 2.49(2.28-3.10) | -3.490c | <0.001 |
| CAL/mm | 2.98(1.63-3.54) | 1.60(1.39-3.10) | -3.965c | <0.001 |
| BOP/% | 27.74(21.36-48.17) | 22.44(17.47-43.03) | -2.600c | 0.009 |
| GI(0~3) | 1.36(0.92-1.88) | 1.07(0.73-1.52) | -2.723c | 0.006 |
| PLI(0~3) | 1.60(1.23-2.25) | 1.37(0.99-1.82) | -2.325c | 0.020 |
| PISA/mm2 | 477.26(27.57-803.55) | 69.61(22.98-451.68) | -3.270c | 0.001 |
| p-tau217/(ng/mL) | 7.00(4.27-9.65) | 2.02(0.80-3.81) | -8.108c | <0.001 |

图 1
血浆p-tau217A:CN组与MCI组间血浆p-tau217水平的比较;B:血浆p-tau217区分MCI与CN的ROC曲线图;C:PD-MIC-、PD+MIC-、PD-MIC+、PD+MIC+4组间血浆p-tau217水平的两两比较;D:CN组的非牙周炎、Ⅰ/Ⅱ牙周炎、Ⅲ/Ⅳ牙周炎患者间血浆p-tau217水平的两两比较;E:MCI组的非牙周炎、Ⅰ/Ⅱ牙周炎、Ⅲ/Ⅳ牙周炎患者间血浆p-tau217水平的两两比较;F:牙周炎与非牙周炎患者间血浆p-tau217水平的比较。

表 2
血浆p-tau217与基线临床因素的相关性分析 (n=192)
| 变量 | 单因素线性回归分析 | 共线性诊断 | ||
|---|---|---|---|---|
| β值 | P值 | 容差 | 方差膨胀因子 | |
| 性别 | 0.198 | 0.731 | ||
| 受教育水平 | 0.068 | 0.540 | ||
| 年龄 | 0.235 | <0.001 | 0.836 | 1.196 |
| 高血压 | 2.499 | <0.001 | 0.398 | 2.511 |
| 吸烟 | 2.678 | <0.001 | 0.719 | 1.392 |
| 饮酒 | 1.344 | 0.036 | 0.755 | 1.325 |
| 体育锻炼 | -1.394 | 0.014 | 0.923 | 1.084 |
| BMI | 0.274 | <0.001 | 0.830 | 1.205 |
| 收缩压 | 0.106 | <0.001 | 0.422 | 2.368 |
| 舒张压 | 0.108 | 0.040 | 0.832 | 1.202 |
| GHbA1c | 2.109 | 0.001 | 0.873 | 1.146 |
| 空腹血糖 | 0.210 | 0.625 | ||
| 总胆固醇 | 0.217 | 0.611 | ||
| 甘油三酯 | 0.696 | 0.219 | ||
| HDL-C | 0.249 | 0.826 | ||
| LDL-C | 1.879 | <0.001 | 0.854 | 1.171 |
| 肌酐 | 0.026 | 0.533 | ||
| eGFR | -0.133 | 0.001 | 0.900 | 1.111 |
| MoCA | -0.767 | <0.001 | 0.263 | 3.807 |
| ADL | 0.654 | <0.001 | 0.322 | 3.106 |
| CDR | 9.024 | <0.001 | 0.154 | 6.490 |
表 3
牙周炎与MCI相关性的多因素Logistic回归分析
| 自变量 | 例数 | 模型1 | 模型2 | 模型3 | 模型4 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| MCI组 | CN组 | OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | OR(95%CI) | P值 | |
| 是否牙周炎 | ||||||||||
| 非牙周炎 | 35 | 54 | 1(参照) | 1(参照) | 1(参照) | 1(参照) | ||||
| 牙周炎 | 61 | 42 | 2.241(1.256~3.998) | 0.006 | 2.153(1.158~4.003) | 0.015 | 2.024(1.074~3.814) | 0.029 | 1.977(1.088~3.594) | 0.025 |
| 牙周炎分期 | ||||||||||
| 非牙周炎 | 35 | 54 | 1(参照) | 1(参照) | 1(参照) | 1(参照) | ||||
| Ⅰ/Ⅱ期 | 35 | 27 | 2.000(1.036~3.862) | 0.039 | 2.082(1.061~4.087) | 0.039 | 1.919(1.055~3.419) | 0.033 | 1.878(1.029~3.425) | 0.040 |
| Ⅲ/Ⅳ期 | 26 | 15 | 2.674(1.245~5.745) | 0.012 | 2.845(1.308~6.188) | 0.008 | 2.747(1.042~7.244) | 0.041 | 2.625(1.073~6.246) | 0.035 |
| Ptrend值 | 0.006 | 0.009 | 0.013 | 0.016 | ||||||
| PISA per 10 mm2 | 96 | 96 | 1.021(1.011~1.031) | <0.001 | 1.018(1.009~1.027) | <0.001 | 1.020(1.010~1.030) | <0.001 | 1.017(1.008~1.026) | <0.001 |
表 4
牙周炎与血浆p-tau217相关性的多元线性回归分析
| 自变量 | 例数 | p-tau217*/(ng/mL) | 模型1 | 模型2 | 模型3 | 模型4 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| β(95%CI) | P值 | β(95%CI) | P值 | β(95%CI) | P值 | β(95%CI) | P值 | |||
| 是否牙周炎 | ||||||||||
| 非牙周炎 | 89 | 1.70(0.80-3.88) | 0(参照) | 0(参照) | 0(参照) | 0(参照) | ||||
| 牙周炎 | 103 | 6.11(3.81-9.22) | 3.753(2.765~4.742) | <0.001 | 3.692(2.722~4.662) | <0.001 | 3.431(2.437~4.425) | <0.001 | 3.309(2.363~4.254) | <0.001 |
| 牙周炎分期 | ||||||||||
| 非牙周炎 | 89 | 1.70(0.80-3.88) | 0(参照) | 0(参照) | 0(参照) | 0(参照) | ||||
| Ⅰ/Ⅱ期 | 62 | 4.63(2.27-7.85) | 2.527(1.454~3.600) | <0.001 | 2.364(1.323~3.404) | <0.001 | 2.121(1.049~3.192) | <0.001 | 1.838(0.869~2.806) | <0.001 |
| Ⅲ/Ⅳ期 | 41 | 8.71(5.28-11.15) | 5.607(4.383~6.831) | <0.001 | 5.651(4.475~6.827) | <0.001 | 5.333(4.131~6.536) | <0.001 | 5.539(4.442~6.636) | <0.001 |
| Ptrend值 | <0.001 | <0.001 | <0.001 | <0.001 | ||||||
| PISA per 10 mm2 | 192 | 4.04(1.22-7.48) | 0.056(0.043~0.069) | <0.001 | 0.055(0.041~0.068) | <0.001 | 0.055(0.043~0.067) | <0.001 | 0.053(0.041~0.066) | <0.001 |
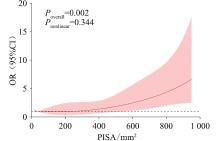
图 3
PISA与MIC间的剂量-反应关系OR为MIC患病风险的比值比;黑色虚线为OR=1的参照线,红线为PISA与MIC相关性的OR值,红色区域为OR值的95%CI。
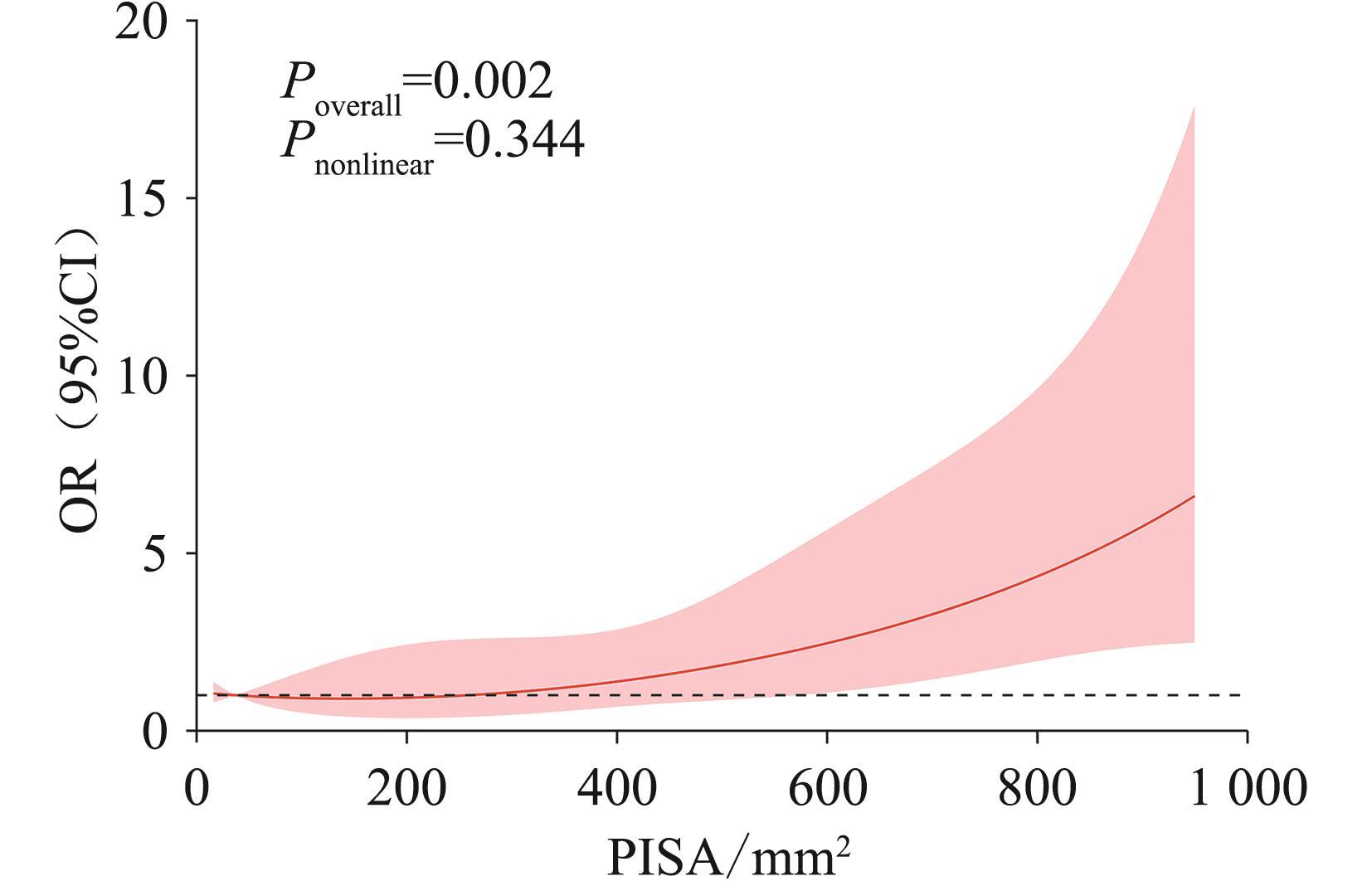
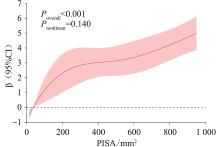
图 4
PISA与血浆p-tau217的剂量-反应关系黑色虚线为β=0的参照线,红线为PISA与血浆p-tau217相关性的β值,红色区域为β值的95%CI。
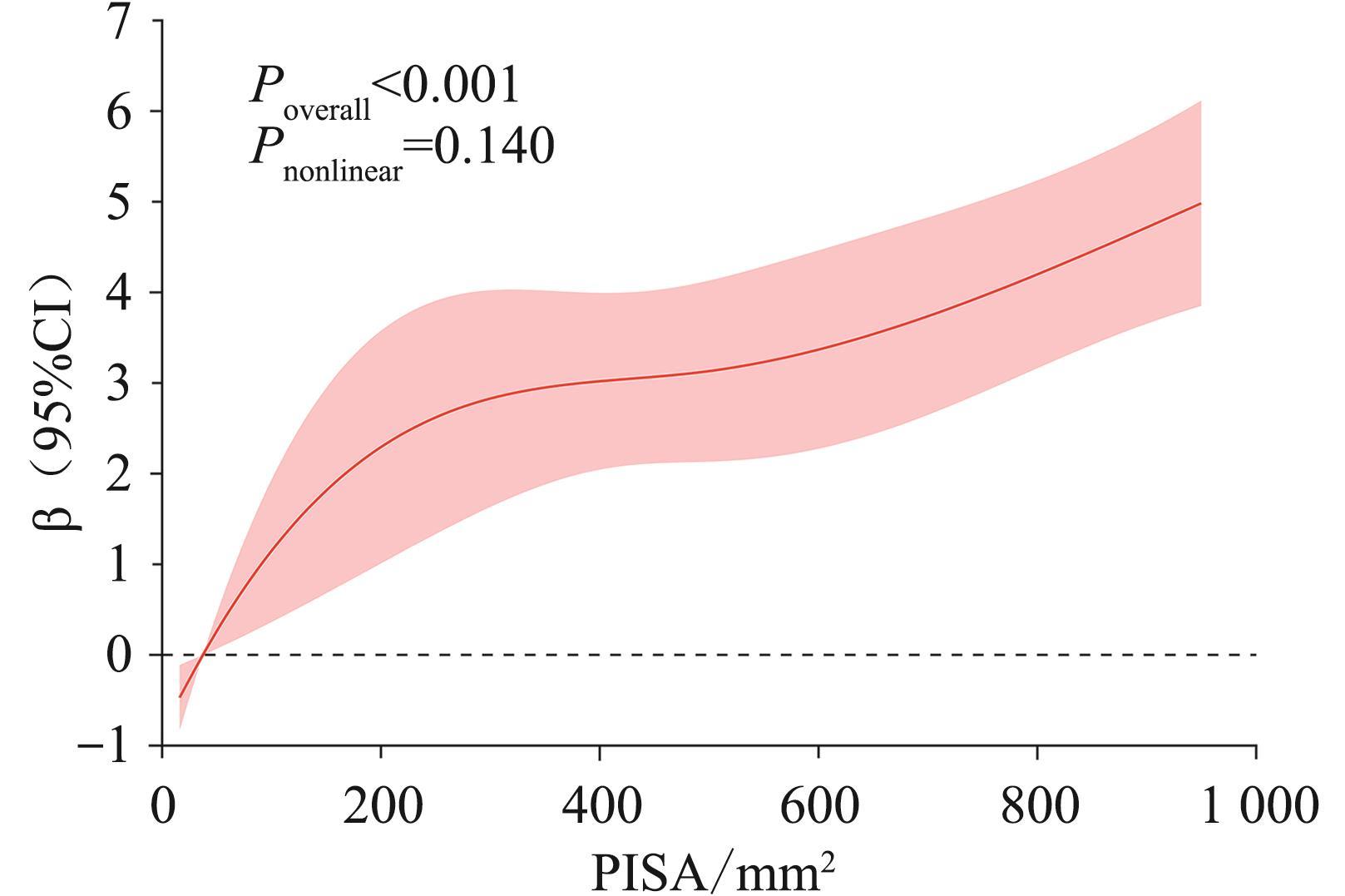
表 5
血浆p-tau217在牙周炎与MCI关联中的中介效应
| 模型 | 总效应 | 直接效应 | 间接效应 | 中介占比 | ||||
|---|---|---|---|---|---|---|---|---|
效应量 (95% Bootstrap CI) | P值 | 效应量 (95% Bootstrap CI) | P值 | 效应量 (95% Bootstrap CI) | P值 | 效应量 (95% Bootstrap CI) | P值 | |
| 模型1 | 0.180(0.038~0.308) | 0.020 | 0.150(0.003~0.282) | 0.044 | 0.031(0.002~0.076) | 0.028 | 17.04%(0.51%~78.31%) | 0.044 |
| 模型2 | 0.195(0.054~0.339) | 0.012 | 0.159(0.013~0.304) | 0.034 | 0.036(0.004~0.086) | 0.014 | 18.57%(1.68%~70.59%) | 0.026 |
| 模型3 | 0.202(0.068~0.332) | 0.004 | 0.169(0.026~0.302) | 0.020 | 0.033(0.005~0.076) | 0.016 | 16.41%(2.39%~61.93%) | 0.020 |
| 模型4 | 0.197(0.057~0.332) | 0.012 | 0.169(0.032~0.307) | 0.024 | 0.028(0.001~0.067) | 0.026 | 13.99%(0.38%~49.39%) | 0.038 |
| [1] | Nasb M, Tao W, Chen N. Alzheimer’s disease puzzle: delving into pathogenesis hypotheses[J]. Aging Dis, 2024, 15(1): 43-73. |
| [2] | Peng L, Bestard-Lorigados I, Song W. The synapse as a treatment avenue for Alzheimer’s Disease[J]. Mol Psychiatry, 2022, 27(7): 2940-2949. |
| [3] | Jia J, Ning Y, Chen M, et al. Biomarker changes during 20 years preceding Alzheimer’s disease[J]. N Engl J Med, 2024, 390(8): 712-722. |
| [4] | Barthélemy NR, Li Y, Joseph-Mathurin N, et al. A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzhei-mer’s disease[J]. Nat Med, 2020, 26(3): 398-407. |
| [5] | Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission[J]. Lancet, 2024, 404(10452): 572-628. |
| [6] | Kiani L. A biomarker for mild cognitive impairment[J]. Nat Rev Neurol, 2023, 19(8): 459. |
| [7] | Mian M, Tahiri J, Eldin R, et al. Overlooked cases of mild cognitive impairment: implications to early Alzhei-mer’s disease[J]. Ageing Res Rev, 2024, 98: 102335. |
| [8] | Li A, Chen Y, van der Sluis LWM, et al. White blood cell count mediates the association between periodontal inflammation and cognitive performance measured by digit symbol substitution test among older U.S. adults[J]. J Gerontol A Biol Sci Med Sci, 2021, 76(7): 1309-1315. |
| [9] | Matsushita K, Yamada-Furukawa M, Kurosawa M, et al. Periodontal disease and periodontal disease-related bacteria involved in the pathogenesis of Alzheimer’s disease[J]. J Inflamm Res, 2020, 13: 275-283. |
| [10] | Hu X, Zhang J, Qiu Y, et al. Periodontal disease and the risk of Alzheimer’s disease and mild cognitive impairment: a systematic review and meta-analysis[J]. Psychogeriatrics, 2021, 21(5): 813-825. |
| [11] | Di Lorenzo D. Tau protein and tauopathies: exploring tau protein-protein and microtubule interactions, cross-interactions and therapeutic strategies[J]. ChemMedChem, 2024, 19(21): e202400180. |
| [12] | Rajendran K, Krishnan UM. Biomarkers in Alzheimer's disease[J]. Clin Chim Acta, 2024, 562: 119857. |
| [13] | Ashton NJ, Brum WS, Di Molfetta G, et al. Diagnostic accuracy of a plasma phosphorylated tau 217 immunoassay for Alzheimer disease pathology[J]. JAMA Neurol, 2024, 81(3): 255-263. |
| [14] | Gonzalez-Ortiz F, Ferreira PCL, González-Escalante A, et al. A novel ultrasensitive assay for plasma p-tau217: Performance in individuals with subjective cognitive decline and early Alzheimer’s disease[J]. Alzheimers Dement, 2024, 20(2): 1239-1249. |
| [15] | Lehmann S, Schraen-Maschke S, Vidal JS, et al. Clinical value of plasma ALZpath pTau217 immunoassay for assessing mild cognitive impairment[J]. J Neurol Neurosurg Psychiatry, 2024, 95(11): 1046-1053. |
| [16] | Jack CR Jr, Andrews JS, Beach TG, et al. Revised criteria for diagnosis and staging of Alzheimer’s disease: Alzheimer’s Association Workgroup[J]. Alzheimers Dement, 2024, 20(8): 5143-5169. |
| [17] | von Elm E, Altman DG, Egger M, et al. The Strengthe-ning the Reporting of Observational Studies in Epide-miology (STROBE) Statement: guidelines for reporting observational studies[J]. Int J Surg, 2014, 12(12): 1495-1499. |
| [18] | Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s di-sease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease[J]. Alzheimers Dement, 2011, 7(3): 270-279. |
| [19] | Fu Z, Zhao M, Wang X, et al. Altered neuroanatomical asymmetries of subcortical structures in subjective cognitive decline, amnestic mild cognitive impairment, and Alzheimer’s disease[J]. J Alzheimers Dis, 2021, 79(3): 1121-1132. |
| [20] | 于丹丹, 周学玲, 牛叠静, 等. 血浆骨桥蛋白水平与2型糖尿病患者合并轻度认知功能障碍的相关性研究[J]. 中华医学杂志, 2024, 104(38): 3593-3599. |
| Yu DD, Zhou XL, Niu DJ, et al. Association between plasma osteopontin level and mild cognitive impairment in patients with type 2 diabetes mellitus[J]. Nat Med J Chin, 2024, 104(38): 3593-3599. | |
| [21] | 中华医学会神经病学分会痴呆与认知障碍学组. 阿尔茨海默病源性轻度认知障碍诊疗中国专家共识2021[J]. 中华神经科杂志, 2022, 55(5): 421-440. |
| Chinese Society of Dementia and Cognitive Impairment. Chinese expert consensus on the diagnosis and treatment of mild cognitive impairment due to Alzheimer’s disease 2021[J]. Chin J Neurol, 2022, 55(5): 421-440. | |
| [22] | Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment[J]. J Am Geriatr Soc, 2005, 53(4): 695-699. |
| [23] | Yu J, Li J, Huang X. The Beijing version of the Montreal Cognitive Assessment as a brief screening tool for mild cognitive impairment: a community-based study[J]. BMC Psychiatry, 2012, 12: 156. |
| [24] | Hong Y, Zeng X, Zhu CW, et al. Evaluating the Beijing version of Montreal Cognitive Assessment for identification of cognitive impairment in monolingual Chinese American older adults[J]. J Geriatr Psychiatry Neurol, 2022, 35(4): 586-593. |
| [25] | Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules[J]. Neurology, 1993, 43(11): 2412-2414. |
| [26] | 中国老年医学学会认知障碍分会. 临床痴呆评定量表简体中文版[J]. 中华老年医学杂志, 2018, 37(4): 367-371. |
| Academy of Cognitive Disorder of China. The Clinical Dementia Rating (simplified Chinese)[J]. Chin J Geriatr, 2018, 37(4): 367-371. | |
| [27] | Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living[J]. Gerontologist, 1969, 9(3): 179-186. |
| [28] | Silness J, Loe H. Periodontal disease in pregnancy. Ⅱ. Correlation between oral hygiene and periodontal condition[J]. Acta Odontol Scand, 1964, 22: 121-135. |
| [29] | Löe H. The gingival index, the plaque index and the retention index systems[J]. J Periodontol, 1967, 38(6): 610-616. |
| [30] | Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque[J]. Int Dent J, 1975, 25(4): 229-235. |
| [31] | Nesse W, Abbas F, van der Ploeg I, et al. Periodontal inflamed surface area: quantifying inflammatory burden[J]. J Clin Periodontol, 2008, 35(8): 668-673. |
| [32] | Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate[J]. Ann Intern Med, 2009, 150(9): 604-612. |
| [33] | Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA)[J]. J Hypertens, 2023, 41(12): 1874-2071. |
| [34] | American Diabetes Association Professional Practice Committee. 2. Diagnosis and Classification of Diabetes: Standards of Care in Diabetes-2024[J]. Diabetes Care, 2024, 47(): S20-S42. |
| [35] | DiseaseKidney: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease[J]. Kidney Int, 2024, 105(4S): S117-S314. |
| [36] | Miller AA, Sharp ES, Wang S, et al. Self-reported hearing loss is associated with faster cognitive and functional decline but not diagnostic conversion in the ADNI cohort[J]. Alzheimers Dement, 2024, 20(11): 7847-7858. |
| [37] | He Q, Li Q, Zhao J, et al. Relationship between plasma lipids and mild cognitive impairment in the elderly Chinese: a case-control study[J]. Lipids Health Dis, 2016, 15(1): 146. |
| [38] | Papapanou PN, Sanz M, Buduneli N,et al.Periodontitis:consensus report of workgroup 2 of the 2017 World Workshop on the classification of periodontal and peri-implant diseases and conditions[J]. J Periodontol, 2018, 89 : S173-S182. |
| [39] | Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition[J]. J Periodontol, 2018, 89 : S159-S172. |
| [40] | Holtfreter B, Kuhr K, Borof K, et al. ACES: a new fra-mework for the application of the 2018 periodontal status classification scheme to epidemiological survey data[J]. J Clin Periodontol, 2024, 51(5): 512-521. |
| [41] | Lin J, Pathak JL, Shen Y, et al. Association between pe-riodontitis and mild cognitive impairment: a systematic review and meta-analysis[J]. Dement Geriatr Cogn Di-sord, 2024, 53(1): 37-46. |
| [42] | Fu YD, Li CL, Hu CL, et al. Meta analysis of the correlation between periodontal health and cognitive impairment in the older population[J]. J Prev Alzheimers Dis, 2024, 11(5): 1307-1315. |
| [43] | Iwasaki M, Kimura Y, Ogawa H, et al. Periodontitis, periodontal inflammation, and mild cognitive impairment: a 5-year cohort study[J]. J Periodontal Res, 2019, 54(3): 233-240. |
| [44] | Carballo Á, López-Dequidt I, Custodia A, et al. Association of periodontitis with cognitive decline and its progression: contribution of blood-based biomarkers of Alzheimer’s disease to this relationship[J]. J Clin Perio-dontol, 2023, 50(11): 1444-1454. |
| [45] | Yamada C, Ho A, Garcia C, et al. Dementia exacerbates periodontal bone loss in females[J]. J Periodontal Res, 2024, 59(3): 512-520. |
| [46] | Fu KL, Chiu MJ, Wara-Aswapati N, et al. Oral micro-biome and serological analyses on association of Alzheimer’s disease and periodontitis[J]. Oral Dis, 2023, 29(8): 3677-3687. |
| [47] | Howe MD, Britton KJ, Joyce HE, et al. Clinical appli-cation of plasma P-tau217 to assess eligibility for amyloid-lowering immunotherapy in memory clinic patients with early Alzheimer’s disease[J]. Alzheimers Res Ther, 2024, 16(1): 154. |
| [48] | Saloner R, VandeVrede L, Asken BM, et al. Plasma phosphorylated tau-217 exhibits sex-specific prognostication of cognitive decline and brain atrophy in cognitively unimpaired adults[J]. Alzheimers Dement, 2024, 20(1): 376-387. |
| [49] | Palmqvist S, Janelidze S, Quiroz YT, et al. Discriminative accuracy of plasma phospho-tau217 for Alzheimer disease vs other neurodegenerative disorders[J]. JAMA, 2020, 324(8): 772-781. |
| [50] | 国家卫生健康委能力建设和继续教育中心, 中国神经科学学会, 衰老标志物联合体, 等. 阿尔茨海默病体液标志物临床应用中国指南(2024 版)[J]. 中华医学杂志, 2024, 104(35): 3292-3306. |
| National Health Commission Capacity Building and Continuing Education Center, Chinese Neuroscience Society, Aging Biomarker Consortium, et al. Chinese gui-deline for clinical application of fluid biomarkers for Alzheimer’s disease(2024 edition)[J]. Nat Med J Chin, 2024, 104(35): 3292-3306. | |
| [51] | Twarowski B, Herbet M. Inflammatory processes in Alzheimer’s disease-pathomechanism, diagnosis and treatment: a review[J]. Int J Mol Sci, 2023, 24(7): 6518. |
| [52] | Shippy DC, Evered AH, Ulland TK. Ketone body metabolism and the NLRP3 inflammasome in Alzheimer’s di-sease[J]. Immunol Rev, 2025, 329(1): e13365. |
| [53] | Sen T, Saha P, Jiang T, et al. Sulfhydration of AKT triggers Tau-phosphorylation by activating glycogen synthase kinase 3β in Alzheimer’s disease[J]. Proc Natl Acad Sci U S A, 2020, 117(8): 4418-4427. |
| [54] | Quintanilla RA, Orellana DI, González-Billault C, et al. Interleukin-6 induces Alzheimer-type phosphorylation of tau protein by deregulating the cdk5/p35 pathway[J]. Exp Cell Res, 2004, 295(1): 245-257. |
| [55] | Wang RP, Huang J, Chan KWY, et al. IL-1β and TNF-α play an important role in modulating the risk of perio-dontitis and Alzheimer’s disease[J]. J Neuroinflammation, 2023, 20(1): 71. |
| [56] | Siew JJ, Chen HM, Chiu FL, et al. Galectin-3 aggravates microglial activation and tau transmission in tauopathy[J]. J Clin Invest, 2024, 134(2): e165523. |
| [57] | Kabacaoğlu B, Öztürk Özener H. Evaluation of inflammasomes as biomarker following non-surgical periodontal treatment[J]. Arch Oral Biol, 2024, 164: 105987. |
| [58] | Sahinkaya S, Yilmaz M, Yay E, et al. Behçet’s disease modifies the gingival inflammatory response[J]. J Periodontol, 2025, 96(4): 321-329. |
| [59] | Chen Y, Yu Y. Tau and neuroinflammation in Alzheimer's disease: interplay mechanisms and clinical translation[J]. J Neuroinflammation, 2023, 20(1): 165. |
| [60] | Jiang M, Zhang X, Yan X, et al. GSK3β is involved in promoting Alzheimer’s disease pathologies following chronic systemic exposure to Porphyromonas gingivalis lipopolysaccharide in amyloid precursor protein NL-F/NL-F knock-in mice[J]. Brain Behav Immun, 2021, 98: 1-12. |
| [61] | Tang Z, Cheng X, Su X, et al. Treponema denticola induces Alzheimer-like tau hyperphosphorylation by activating hippocampal neuroinflammation in mice[J]. J Dent Res, 2022, 101(8): 992-1001. |
| [62] | Yan C, Diao Q, Zhao Y, et al. Fusobacterium nucleatum infection-induced neurodegeneration and abnormal gut microbiota composition in Alzheimer’s disease-like rats[J]. Front Neurosci, 2022, 16: 884543. |
| [1] | 陈兰, 朱轩智, 周婕妤, 李继遥, 赵蕾. 龈沟液中细胞外游离DNA与牙周临床指标及环磷酸鸟苷—磷酸腺苷合成酶—干扰素基因刺激因子信号通路相关分子的关联性分析[J]. 华西口腔医学杂志, 2025, 43(6): 808-818. |
| [2] | 郭梦茹, 张天翼, 黄靖雯, 黄莘越, 郑义, 张莉. 墨旱莲—女贞子治疗牙周炎的潜在成分及作用机制[J]. 华西口腔医学杂志, 2025, 43(5): 696-710. |
| [3] | 李华, 张康, 曲会娟, 冀洪海, 孙敏敏. 人参皂苷Rb3对大鼠实验性牙周炎的疗效研究[J]. 华西口腔医学杂志, 2025, 43(5): 711-721. |
| [4] | 张雪颖, 孟鑫, 刘志臻, 张康, 冀洪海, 孙敏敏. 人参皂苷Rb3调节磷酸化细胞外信号调节激酶通路减轻牙周炎大鼠炎症反应促进成骨[J]. 华西口腔医学杂志, 2025, 43(2): 236-248. |
| [5] | 冯苗苗, 徐小苒, 李宁丽, 杨铭真, 翟远坤. 基于网络药理、分子对接和分子动力学模拟探讨蛇床子治疗牙周炎伴骨质疏松的作用机制[J]. 华西口腔医学杂志, 2025, 43(2): 249-261. |
| [6] | 付岚清, 郝新宇, 钱文博, 孙颖. 基础治疗对重度牙周炎患者龈沟液内中性粒细胞胞外诱捕网形成的影响研究[J]. 华西口腔医学杂志, 2025, 43(1): 46-52. |
| [7] | 陈宇翔, 赵安娜, 杨浩然, 杨霞, 程婷婷, 饶先琦, 李自良. 基于机器学习和生物信息学分析的脂肪酸代谢相关基因在牙周炎中的作用研究[J]. 华西口腔医学杂志, 2024, 42(6): 735-747. |
| [8] | 周露露, 滕念, 高甜甜, 王洪斌, 高翔. 香芹酚水凝胶对牙周炎大鼠牙槽骨保护作用研究[J]. 华西口腔医学杂志, 2024, 42(5): 593-608. |
| [9] | 李琼, 马浩楠, 商雅琦, 辛禧瑞, 刘歆婵, 武洲, 于维先. 线粒体解偶联蛋白2在大鼠实验性牙周炎相关肾损伤中的作用研究[J]. 华西口腔医学杂志, 2024, 42(4): 502-511. |
| [10] | 杨荣霞, 宗颖睿, 张晨. 慢性牙周炎与帕金森病之间潜在相关性的初探[J]. 华西口腔医学杂志, 2024, 42(4): 521-530. |
| [11] | 李钺, 许春梅, 谢旭东, 施培磊, 王骏, 丁一. 骨膜蛋白在小鼠牙周炎进程中的时空表达规律研究[J]. 华西口腔医学杂志, 2024, 42(3): 286-295. |
| [12] | 辛雨, 傅若冰, 辛禧瑞, 商雅琦, 刘歆婵, 于维先. 缝隙连接蛋白43通过调控凋亡参与大鼠牙周炎相关肾损伤[J]. 华西口腔医学杂志, 2024, 42(3): 296-303. |
| [13] | 马浩楠, 李琼, 商雅琦, 辛禧瑞, 刘歆婵, 武洲, 于维先. 生物钟蛋白Bmal1对实验性牙周炎相关肾损伤的影响[J]. 华西口腔医学杂志, 2024, 42(2): 163-171. |
| [14] | 孙金梦, 张颖, 郑泽君, 丁晓玲, 孙敏敏, 丁刚. 基于网络药理学和分子对接技术探讨人参对牙周炎的潜在治疗机制[J]. 华西口腔医学杂志, 2024, 42(2): 181-191. |
| [15] | 叶畅畅, 杨禾, 黄萍. 意向性牙再植术保留重度牙周炎患牙的临床应用策略[J]. 华西口腔医学杂志, 2024, 42(1): 12-18. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||

