| 1 |
Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations[J]. Int J Oral Maxillofac Implants, 2004, 19(): 43-61.
|
| 2 |
Monje A, Galindo-Moreno P, Tözüm TF, et al. Into the paradigm of local factors as contributors for peri-implant disease: short communication[J]. Int J Oral Maxillofac Implants, 2016, 31(2): 288-292.
|
| 3 |
Canullo L, Tallarico M, Radovanovic S, et al. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis[J]. Clin Oral Implants Res, 2016, 27(10): 1243-1250.
|
| 4 |
Choi W, Nguyen BC, Doan A, et al. Freehand versus gui-ded surgery: factors influencing accuracy of dental implant placement[J]. Implant Dent, 2017, 26(4): 500-509.
|
| 5 |
Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest[J]. J Periodontol, 2000, 71(4): 546-549.
|
| 6 |
Greenstein G, Cavallaro J, Romanos G, et al. Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry: a review[J]. J Periodontol, 2008, 79(8): 1317-1329.
|
| 7 |
Chan HL, Benavides E, Yeh CY, et al. Risk assessment of lingual plate perforation in posterior mandibular region: a virtual implant placement study using cone-beam computed tomography[J]. J Periodontol, 2011, 82(1): 129-135.
|
| 8 |
Chan HL, Garaicoa-Pazmino C, Suarez F, et al. Incidence of implant buccal plate fenestration in the esthetic zone: a cone beam computed tomography study[J]. Int J Oral Maxillofac Implants, 2014, 29(1): 171-177.
|
| 9 |
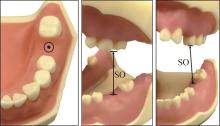
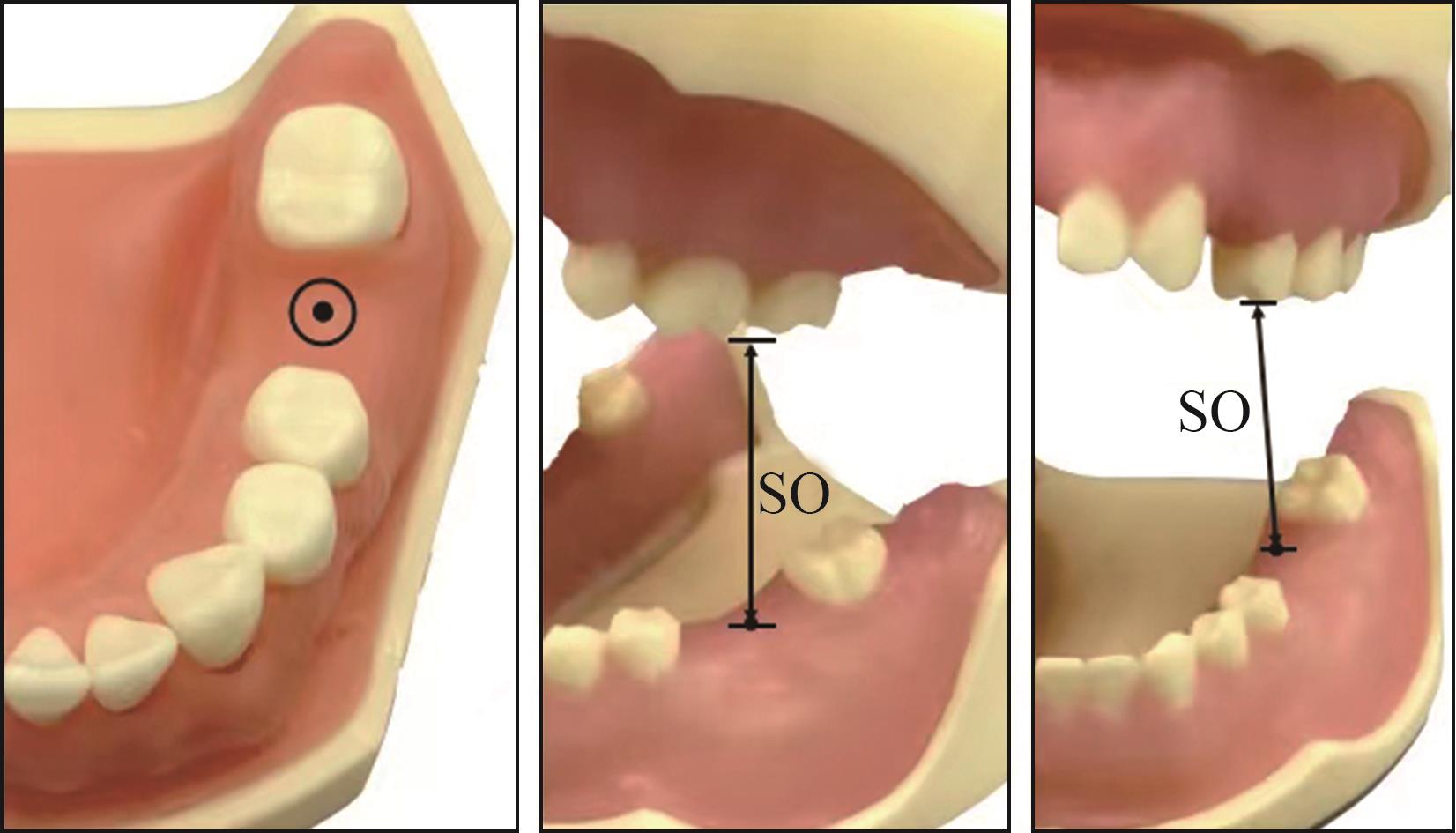
张婧, 张淑宁, 张静, 等. 开口度及牙弓长度、宽度对11#~14#Gracey刮治器使用的影响[J]. 实用口腔医学杂志, 2020, 36(4): 609-612.
|
|
Zhang J, Zhang SN, Zhang J, et al. The influences of mouth opening, the length and width of dental arch on the use of Gracey curettes[J]. J Pract Stomatol, 2020, 36(4): 609-612.
|
| 10 |
Kumar B, Fernandes A, Sandhu PK. Restricted mouth opening and its definitive management: a literature review[J]. Indian J Dent Res, 2018, 29(2): 217-224.
|
| 11 |
Noharet R, Pettersson A, Bourgeois D. Accuracy of implant placement in the posterior maxilla as related to 2 types of surgical guides: a pilot study in the human cadaver[J]. J Prosthet Dent, 2014, 112(3): 526-532.
|
| 12 |
Fang Y, An X, Jeong SM, et al. Accuracy of computer-guided implant placement in anterior regions[J]. J Prosthet Dent, 2019, 121(5): 836-842.
|
| 13 |
D'haese J, Ackhurst J, Wismeijer D, et al. Current state of the art of computer-guided implant surgery[J]. Periodontol 2000, 2017, 73(1): 121-133.
|
| 14 |
Lin WS, Yang CC, Polido WD, et al. CAD-CAM cobalt-chromium surgical template for static computer-aided implant surgery: a dental technique[J]. J Prosthet Dent, 2020, 123(1): 42-44.
|

 ), 吴嘉诚, 胡楠
), 吴嘉诚, 胡楠