West China Journal of Stomatology ›› 2023, Vol. 41 ›› Issue (4): 434-442.doi: 10.7518/hxkq.2023.2022495
• Clinical Research • Previous Articles Next Articles
Wang Tiebiao( ), Zhou Wuchao, Xiao Yin, Cheng Jialong, Ouyang Zhoucheng, Cheng Chen, Xi Weihong.()
), Zhou Wuchao, Xiao Yin, Cheng Jialong, Ouyang Zhoucheng, Cheng Chen, Xi Weihong.()
Received:2022-12-24
Revised:2023-04-09
Online:2023-08-01
Published:2023-07-21
Contact:
Xi Weihong.
E-mail:307334636@qq.com;xwh1975@163.com
Supported by:CLC Number:
Wang Tiebiao, Zhou Wuchao, Xiao Yin, Cheng Jialong, Ouyang Zhoucheng, Cheng Chen, Xi Weihong.. Application of modified articular disc anchorage in treating the perforation and rupture of temporomandibular joint disc[J]. West China Journal of Stomatology, 2023, 41(4): 434-442.
Add to citation manager EndNote|Ris|BibTeX
Fig 1
Schematic diagram of the classification of articular disc perforations
Fig 2
Different types of temporomandibular joint disc perforation


Fig 3
Condition of incision
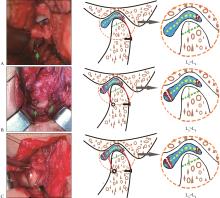
Fig 4
Modified articular disc anchorage

Tab 1
Clinical function examination results before treatment and 1, 3, 6 months after treatment of patients
| 时间 | VAS | MIO/mm | CMI |
|---|---|---|---|
| 术前 | 6.33±2.30 | 22.00±8.20 | 0.426±0.111 |
| 术后1个月 | 3.50±1.47① | 23.72±4.94② | 0.335±0.077③ |
| 术后3个月 | 1.50±1.34① | 30.50±3.92① | 0.162±0.09① |
| 术后6个月 | 0.44±0.62① | 34.44±4.44① | 0.133±0.108① |

Fig 5
Preoperative and postoperative MRI results in oblique sagittal position of different surgical methods

| 1 | 龙星. 颞下颌关节盘穿孔的外科治疗[J]. 中华口腔医学杂志, 2005, 40(5): 423-424. |
| Long X. Surgical treatment of temporomandibular joint disc perforation[J]. Chin J Stomatol, 2005, 40(5): 423-424. | |
| 2 | Fricton JR, Schiffman EL. The craniomandibular index: validity[J]. J Prosthet Dent, 1987, 58(2): 222-228. |
| 3 | Holmlund AB. Surgery for TMJ internal derangement. Evaluation of treatment outcome and criteria for success[J]. Int J Oral Maxillofac Surg, 1993, 22(2): 75-77. |
| 4 | 恽白, 俞蕾蕾, 罗怡. 颞下颌关节镜治疗关节盘前移伴穿孔患者的全程康复护理探讨[J]. 中国口腔颌面外科杂志, 2020, 18(6): 531-534. |
| Yun B, Yu LL, Luo Y. Full-time rehabilitation nursing in arthroscopic discopexy for anterior disc displacement with perforation of temporomandibular joint[J]. China J Oral Maxillofac Surg, 2020, 18(6): 531-534. | |
| 5 | Machon V, Levorova J, Hirjak D, et al. Temporomandibular joint disc perforation: a retrospective study[J]. Int J Oral Maxillofac Surg, 2017, 46(11): 1411-1416. |
| 6 | 詹翔. 颞下颌关节有限元模型的生物力学特征[J]. 中国组织工程研究, 2018, 22(20): 3172-3177. |
| Zhan X. Biomechanical properties of the finite element model of temporomandibular joint[J]. Chin J Tissue Eng Res, 2018, 22(20): 3172-3177. | |
| 7 | Nitzan DW. The process of lubrication impairment and its involvement in temporomandibular joint disc displa-cement: a theoretical concept[J]. J Oral Maxillofac Surg, 2001, 59(1): 36-45. |
| 8 | Narinobou M, Takatsuka S, Nakagawa K, et al. Histological changes in the rabbit condyle following posterolateral disk perforation[J]. J Craniomaxillofac Surg, 2000, 28(6): 345-351. |
| 9 | 张颖, 冯梓峻, 黎星阳, 等. 基于CBCT下颞下颌关节造影的关节盘穿孔与髁突骨质改变相关性研究[J]. 口腔医学研究, 2020, 36(4): 333-336. |
| Zhang Y, Feng ZJ, Li XY, et al. Correlation between disc perforation and condylar bone changes based on temporomandibular joint arthrography by CBCT[J]. J Oral Sci Res, 2020, 36(4): 333-336. | |
| 10 | 张海捷, 殷夫, 李烨铭, 等. 探讨MRI对颞下颌关节紊乱病中关节盘穿孔的诊断标准[J]. 临床放射学杂志, 2021, 40(1): 30-35. |
| Zhang HJ, Yin F, Li YM, et al. To explore the criteria of MRI in the diagnosis of disc perforation in temporomandibular disorders[J]. J Clin Radiol, 2021, 40(1): 30-35. | |
| 11 | Verhelst PJ, Vervaeke K, Orhan K, et al. The agreement between magnetic resonance imaging and arthroscopic findings in temporomandibular joint disorders[J]. Int J Oral Maxillofac Surg, 2021, 50(5): 657-664. |
| 12 | Mazzonetto R, Spagnoli DB. Long-term evaluation of arthroscopic discectomy of the temporomandibular joint using the Holmium YAG laser[J]. J Oral Maxillofac Surg, 2001, 59(9): 1018-1023. |
| 13 | Baheerathan NN, Sayan A, Demir E, et al. Outcome of eminectomy combined with discectomy and silastic interpositional graft for temporomandibular joint dysfunction: a retrospective study of 20 years[J]. Br J Oral Maxillofac Surg, 2020, 58(7): 854-860. |
| 14 | Takaku S, Toyoda T. Long-term evaluation of discectomy of the temporomandibular joint[J]. J Oral Maxillofac Surg, 1994, 52(7): 722-728. |
| 15 | 杨驰, 邱蔚六, 陈敏洁, 等. 自体耳廓软骨瓣置换或重建颞下颌关节盘: 临床疗效评价[J]. 口腔颌面外科杂志, 2000, 10(2): 124-127. |
| Yang C, Qiu WL, Chen MJ, et al. Autogenous auricular cartilage graft for disc replacement or reconstruction of the temporomandibular joint. A clinical study[J]. J Oral Maxillofac Surg, 2000, 10(2): 124-127. | |
| 16 | 陈光灿, 陈敏洁, 杨驰, 等. 带蒂颞深筋膜脂肪瓣在颞下颌关节重建中的应用: 135例临床分析[J]. 中国口腔颌面外科杂志, 2020, 18(5): 412-416. |
| Chen GC, Chen MJ, Yang C, et al. Application of pedicled deep temporal fascial fat flap in temporomandibular joint reconstruction: clinical analysis of 135 consecutive cases[J]. China J Oral Maxillofac Surg, 2020, 18(5): 412-416. | |
| 17 | DeMerle M, Nafiu OO, Aronovich S. Temporomandibular joint discectomy with abdominal fat graft versus temporalis myofascial flap: a comparative study[J]. J Oral Maxillofac Surg, 2017, 75(6): 1137-1143. |
| 18 | Machoň V, Vir J, Levorová J, et al. Discectomy with subsequent free fat flap insertion in disc perforation therapy of temporomandibular joint. Assessment of results 24 months after operation[J]. Prague Med Rep, 2020, 121(2): 96-106. |
| 19 | 邓末宏, 龙星, 李健, 等. 手术治疗颞下颌关节盘穿孔的临床研究[J]. 中华口腔医学研究杂志(电子版), 2008, 2(1): 52-56. |
| Deng MH, Long X, Li J, et al. A clinical study of surgical treatment with temporomandibular joint disc perforation[J]. Chin J Stomatol Res (Electron Ed), 2008, 2(1): 52-56. | |
| 20 | 肖勉, 胡智慧, 江恒华, 等. 破骨细胞分化在颞下颌关节骨关节炎发生中的作用[J]. 华西口腔医学杂志, 2021, 39(4): 398-404. |
| Xiao M, Hu ZH, Jiang HH, et al. Role of osteoclast differentiation in the occurrence of osteoarthritis of temporomandibular joint[J]. West China J Stomatol, 2021, 39(4): 398-404. | |
| 21 | 何冬梅, 张露珠, 杨驰. 国产人工颞下颌关节的研发和初步临床应用[J]. 中华口腔医学杂志, 2017, 52(4): 232-237. |
| He DM, Zhang LZ, Yang C. Development and preliminary clinical application of home-made temporomandibular joint prostheses[J]. Chin J Stomatol, 2017, 52(4): 232-237. | |
| 22 | Arab K, Alfaqeeh FA, Danino MA. Internal derangement of temporomandibular joint: umbrella perforated screw technique[J]. J Family Med Prim Care, 2021, 10(2): 652-656. |
| 23 | 张善勇, 张晓虎, 霍亮, 等. 改良颞下颌关节盘锚固术—技术介绍[J]. 中国口腔颌面外科杂志, 2012, 10(6): 478-483. |
| Zhang SY, Zhang XH, Huo L, et al. Modified temporomandibular joint disc anchor: technical notes[J]. China J Oral Maxillofac Surg, 2012, 10(6): 478-483. | |
| 24 | 沈达, 李健. 可吸收带线锚固钉与金属锚固钉治疗颞下颌关节盘不可复性前移位的短期疗效比较[J]. 口腔颌面外科杂志, 2022, 32(1): 55-59. |
| Shen D, Li J. Comparative study on the short-term efficacy of bio-absorbable anchoring nails vs metallic anchoring nails for the treatment of TMJ anterior disc displacement without reduction[J]. J Oral Maxillofac Surg, 2022, 32(1): 55-59. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 This work is licensed under a Creative Commons Attribution 3.0 License.
This work is licensed under a Creative Commons Attribution 3.0 License.
