West China Journal of Stomatology ›› 2025, Vol. 43 ›› Issue (1): 106-113.doi: 10.7518/hxkq.2024.2024207
• Clinical Research • Previous Articles Next Articles
Wang Zeyu( ), Du Chongli, Wang Dong, Peng Xiao, Du Yue, Wang Hanying, Gao Tingyi, Han Rui, Zhang Kai()
), Du Chongli, Wang Dong, Peng Xiao, Du Yue, Wang Hanying, Gao Tingyi, Han Rui, Zhang Kai()
Received:2024-05-24
Revised:2024-08-22
Online:2025-02-01
Published:2025-01-22
Contact:
Zhang Kai
E-mail:wzy13170025087@163.com;zk29788@163.com;k29788@163.com
Supported by:CLC Number:
Wang Zeyu, Du Chongli, Wang Dong, Peng Xiao, Du Yue, Wang Hanying, Gao Tingyi, Han Rui, Zhang Kai. A retrospective study of the effects of different surgical procedures on the mandibular nerve canal involved by odontogenic keratocyst[J]. West China Journal of Stomatology, 2025, 43(1): 106-113.
Add to citation manager EndNote|Ris|BibTeX
Tab 1
Comparison of general data between the two groups
| 项目 | A组 | B组 | t或x2值 | P值 |
|---|---|---|---|---|
| 性别/n | 0.102 | 0.749 | ||
| 男 | 12 | 11 | ||
| 女 | 8 | 9 | ||
| 年龄/岁 | 30.60±10.94 | 38.9±18.82 | 157.5 | 0.249 |
| 囊肿最大径/cm | 3.90±0.41 | 3.91±0.41 | 198.5 | 0.968 |
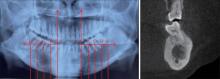
Fig 1
Measurement method of mandibular nerve canal related data

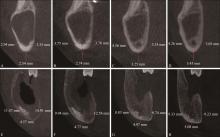
Fig 2
Changes in the position of the mandibular nerve canal

Fig 3
Changes in displacement of the neural tube in the vertical direction
Tab 2
Displacement of the MC in the vertical direction
| 时间 | A组/mm | B组/mm | 置信区间(95%CI) | t值 | P值 |
|---|---|---|---|---|---|
| 术后9个月总位移 | 1.03±0.17 | 0.52±0.10 | 0.52(0.37,0.67) | 9.17 | 0.000 1 |
| 术后0~3个月位移 | 0.25±0.03 | 0.19±0.02 | 0.06(0.04,0.08) | 8.74 | 0.000 1 |
| 术后3~6个月位移 | 0.54±0.08 | 0.23±0.07 | 0.31(0.26,0.36) | 11.27 | 0.000 1 |
| 术后6~9个月位移 | 0.24±0.21 | 0.10±0.05 | 0.15(0.01,0.29) | 2.37 | 0.039 0 |
Tab 3
Displacement of the mandibular nerve canal in the buccolingual direction
| H值 | A组/mm | B组/mm | 置信区间(95% CI) | t值 | P值 |
|---|---|---|---|---|---|
| 手术前 | 0.86±0.05 | 0.82±0.07 | 0.03(0.01,0.08) | 0.81 | 0.422 9 |
| 术后3个月 | 1.02±0.07 | 0.89±0.06 | 0.14(0.08,0.20) | 5.06 | 0.000 1 |
| 术后6个月 | 1.27±0.10 | 0.93±0.05 | 0.34(0.28,0.36) | 13.85 | 0.000 1 |
| 术后9个月 | 1.35±0.03 | 1.04±0.06 | 0.31(0.26,0.35) | 15.40 | 0.000 1 |
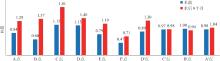
Fig 4
Changes in H values over time at different observation points

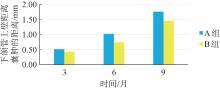
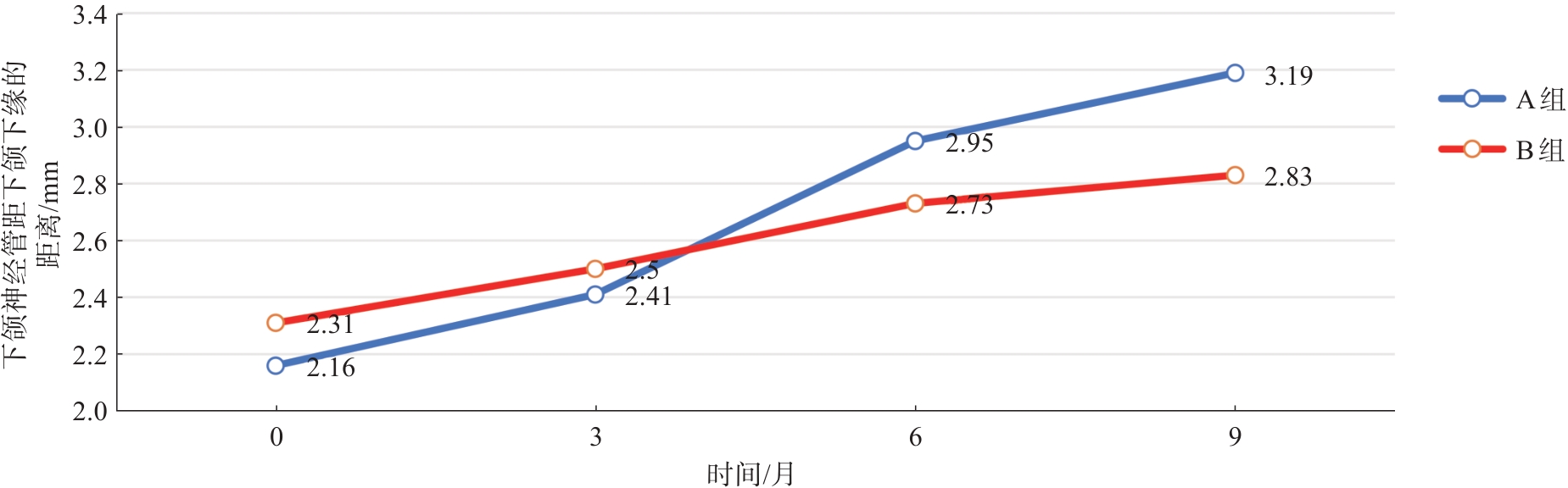
Fig 5
Distance between the upper wall of cyst at the closest points of mandibular nerve canal and the cyst
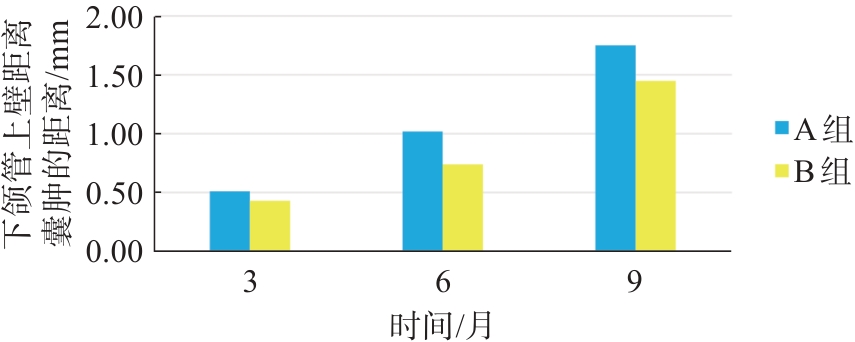

Fig 6
Recovery of the upper wall of the MC on the side of the window opening

Tab 4
Distance between the upper wall of the mandibular canal and the cyst after surgery
| 时间 | MC距囊肿距离/mm | t值 | P值 | |
|---|---|---|---|---|
| 术后3个月 | A组 | 0.51±0.10 | 0.588 | 0.56 |
| B组 | 0.43±0.09 | |||
| 术后6个月 | A组 | 1.02±0.19 | 1.864 | 0.07 |
| B组 | 0.74±0.16 | |||
| 术后9个月 | A组 | 1.75±0.15 | 2.601 | 0.01 |
| B组 | 1.45±0.09 | |||
| 1 | Rajendra Santosh AB. Odontogenic cysts[J]. Dental Clin North Am, 2020, 64(1): 105-119. |
| 2 | 邸瑞玲, 李向春, 张鑫, 等. 应用袋形术联合囊肿塞治疗大型颌骨囊肿临床疗效分析[J]. 口腔颌面外科杂志, 2018, 28(6): 338-340. |
| Di RL, Li XC, Zhang X, et al. Marsupialization combined with cyst plug on the treatment of large cyst of jaw. A clinical review of 39 cases[J]. J Oral Maxillofac Surg, 2018, 28(6): 338-340. | |
| 3 | Singh AK, Khanal N, Chaulagain R, et al. How effective is 5-Fluorouracil as an adjuvant in the management of odontogenic keratocyst? A systematic review and meta-analysis[J]. Br J Oral Maxillofac Surg, 2022, 60(6): 746-754. |
| 4 | Evangelista K, Cardoso L, Toledo Í, et al. Directions of mandibular canal displacement in ameloblastoma: a com-puted tomography mirrored-method analysis[J]. Imaging Sci Dent, 2021, 51(1): 17-25. |
| 5 | Vered M, Wright JM. Update from the 5th edition of the World Health Organization classification of head and neck tumors: odontogenic and maxillofacial bone tumours[J]. Head Neck Pathol, 2022, 16(1): 63-75. |
| 6 | 王鹏程, 陈春晖, 童熹, 等. β-TCP植入与口腔修复膜覆盖治疗对颌骨囊肿术后骨缺损的修复效果分析[J]. 口腔医学研究, 2021, 37(3): 260-263. |
| Wang PC, Chen CH, Tong X, et al. Effect of β-TCP combined with oral repair membrane on bone defect restoration after jaw cyst excision[J]. Oral Med Res, 2021, 37(3): 260-263. | |
| 7 | Han YS, Lee H, Seo BM. Fate of mandibular canals displaced by enlarged cystic lesions: does the inferior alveolar neurovascular bundle relocate to its original position[J]. Br J Oral Maxillofac Surg, 2018, 56(4): 292-298. |
| 8 | Ku JK, Han M, Yongvikul A, et al. Volumetric analysis of spontaneous bone healing after jaw cyst enucleation[J]. Sci Rep, 2022, 12(1): 14953. |
| 9 | Wine WM, Welch JT, Graves RW. Marsupialization of a dentigerous cyst of the mandible: report of case[J]. J Oral Surg, 1971, 29(10): 742-745 |
| 10 | 章茜, 杨旭东. 颌骨囊性病变开窗减压术疗效评价方法的研究进展[J]. 国际口腔医学杂志, 2017, 44(4): 493-496. |
| Zhang Q, Yang XD. Research progress on the effectiveness assessment of decompression on large jaw cystic lesions[J]. Int J Stomatol, 2017, 44(4): 493-496. | |
| 11 | 肖锋, 薛浩伟, 方冬冬, 等. 超声骨刀技术联合医用胶原蛋白海绵在颌骨囊肿中的应用[J]. 临床口腔医学杂志, 2022, 38(7): 430-433. |
| Xiao F, Xue HW, Fang DD, et al. Study on the therapeutic effect of ultrasonic bone knife combined with medical collagen sponge in patients with jaw cyst and its effect on inflammatory factors[J]. J Clin Stomatol, 2022, 38(7): 430-433. | |
| 12 | 庞亚倩, 张凯, 刘亮, 等. 下颌骨囊性病变的三维有限元模型生物力学分析[J]. 南方医科大学学报, 2020, 40(6): 911-915. |
| Pang YQ, Zhang K, Liu L, et al. Biomechanical analysis of three-dimensional finite element model of mandibular cystic lesions[J]. J Southern Med Univ, 2020, 40(6): 911-915. | |
| 13 | 彭笑, 张晨晨, 韩瑞, 等. 未成年人大型囊性成釉细胞瘤序列法治疗临床研究[J]. 实用口腔医学杂志, 2023, 39(2): 236-242. |
| Peng X, Zhang CC, Han R, et al. Clinical study of sequential treatment of large cystic ameloblastoma in minors[J]. J Pract Stomatol, 2023, 39(2): 236-242. | |
| 14 | Nakamura N, Mitsuyasu T, Mitsuyasu Y, et al. Marsupia-lization for odontogenic keratocysts: long-term follow-up analysis of the effects and changes in growth characteristics[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2002, 94(5): 543-553. |
| 15 | Singh AK, Khanal N, Chaulagain R, et al. How effective is 5-Fluorouracil as an adjuvant in the management of odontogenic keratocyst? A systematic review and meta-analysis[J]. Br J Oral Maxillofac Surg, 2022, 60(6): 746-754. |
| 16 | Cho JY, Kim JW, Kim SB, et al. Decompression of large cyst invading the mandibular canal leading to reduced cyst volume and increased mandibular canal length[J]. J Oral Maxillofac Surg, 2020, 78(10): 1770-1779. |
| 17 | Vranckx M, Geerinckx H, Gaêta-Araujo H, et al. Do anatomical variations of the mandibular canal pose an increased risk of inferior alveolar nerve injury after third molar removal[J]. Clin Oral Investig, 2022, 26(1): 931-937. |
| 18 | Li Y, Li L, Shi J, et al. Positional changes of mandibular canal before and after decompression of cystic lesions in the mandible[J]. J Oral Maxillofac Surg, 2021, 79(4): 854-862. |
| 19 | Liu T, Xia B, Gu Z. Inferior alveolar canal course: a radiographic study[J]. Clin Oral Implants Res, 2009, 20(11): 1212-1218. |
| 20 | 杜悦, 彭笑, 韩瑞, 等. 颌骨囊肿开窗治疗临床特征动态研究[J]. 上海口腔医学, 2021, 30(6): 658-662. |
| Du Y, Peng X, Han R, et al. Clinical dynamic study of jaw cyst after decompression[J]. Shanghai J Stomatol, 2021, 30(6): 658-662. | |
| 21 | Al-Moraissi EA, Kaur A, Gomez RS, et al. Effectiveness of different treatments for odontogenic keratocyst: a network meta-analysis[J]. Int J Oral Maxillofac Surg, 2023, 52(1): 32-43. |
| 22 | Hoshi R, Tetsumura A, Yamaguchi S. Preoperative ima-ging findings as predictors of postoperative inferior al-veolar nerve injury following mandibular cyst surgery[J]. J Oral Sci, 2018, 60(4): 618-625. |
| 23 | Etoz OA, Er N, Demirbas AE. Is supraperiosteal infiltration anesthesia safe enough to prevent inferior alveolar nerve during posterior mandibular implant surgery[J]. Med Oral Patol Oral Cir Bucal, 2011, 16(3): e386-e389. |
| 24 | Başa O, Dilek OC. Assessment of the risk of perforation of the mandibular canal by implant drill using density and thickness parameters[J]. Gerodontology, 2011, 28(3): 213-220. |
| [1] | Xu Chen, Chang Hongguang, Shao Qiang, Song Yonghai. Conservative treatment of pathological fracture after multiple odontogenic keratocyst surgery: a case report and literature analysis [J]. West China Journal of Stomatology, 2025, 43(1): 144-150. |
| [2] | Chen Meiyu, Tao Shicheng, Chen Guosheng, Tang Yiyao, Mai Huaming.. Nevoid basal cell carcinoma syndrome with anophthalmia: a case report [J]. West China Journal of Stomatology, 2022, 40(2): 240-245. |
| [3] | Liu Wei, Li Honglin, Xiang Sijie, Miao Cheng, Li Chunjie, Han Bo. Peripheral odontogenic keratocysts in buccal soft tissues: two cases report [J]. West China Journal of Stomatology, 2021, 39(6): 728-731. |
| [4] | Tian Ziyi, Ma Wen, Zhao Zhiyue, Li Ming. Basal cell nevus syndrome with Duchenne muscular dystrophy: a case report [J]. West China Journal of Stomatology, 2021, 39(2): 230-232. |
| [5] | Liu Yixiu, Qu Yang, Li Zhenhua, Wang Hongpeng. Effect of decompression combined with curettage and autogenous bone cement implantation on large cysts of the jaw [J]. West China Journal of Stomatology, 2020, 38(4): 464-469. |
| [6] | Yu Yongchun, Yu Weiming, Yang Zhengyi, Zhang Shubiao, Sun Jie, Liu Lei. Left lower extremity venous thrombosis after operation of cyst in the jaw: a case report [J]. West China Journal of Stomatology, 2014, 32(2): 203-205. |
| [7] | Zhang Guimei, Wang Tao, Mao Xiaobin, Yang Dongkun.. CT morphology of mandibular bone and mandibular nerve canal in hemimandibular elongation [J]. West China Journal of Stomatology, 2012, 30(2): 152-155. |
| [8] | ZHOU Shang- hui1, LI Li- li2, JIAN Xin- chun1, JIANG Can- hua1. A case of nevoid basal cell car cinoma syndrome family [J]. West China Journal of Stomatology, 2008, 26(01): 109-111. |
| [9] | LU Da- peng1, XING Ru- dong2, SHU Ping1, TANG Xiao- fei3, ZHANG Min1. Cytoker atin 18 and Their Gene Expr ession in Jaw Odontogenic Ker atocyst Epithelial Lining [J]. West China Journal of Stomatology, 2007, 25(02): 106-110. |
| [10] | ZHAO Ning1, GE Shao-hua1, DING Guang-yao2. Clinical Effect of Minocycline as Adjunctive Therapy to Scaling and Root Planning on Treatment of Chronic Periodontitis [J]. West China Journal of Stomatology, 2006, 24(01): 32-35. |
| [11] | ZHONG Ming1,LI Zi-juan1,WANG Jie1,ZHANG Bo2,HOULin2,GONG Yan-bing1. Expression of Telomerase Activity and c-myc and Stimulatory Protein 1 in Human Ameloblastoma [J]. West China Journal of Stomatology, 2004, 22(06): 499-502. |
| [12] | Jiang Ziqiang, Zhao Yifang. A Comparative Study of Suction Drainage and Decompression in the Treatment of Odontogenic Keratocysts [J]. West China Journal of Stomatology, 2002, 20(04): 265-267. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 This work is licensed under a Creative Commons Attribution 3.0 License.
This work is licensed under a Creative Commons Attribution 3.0 License.
