West China Journal of Stomatology ›› 2023, Vol. 41 ›› Issue (1): 43-51.doi: 10.7518/hxkq.2023.01.006
Previous Articles Next Articles
Feng Zhiqiang1,2,3( ), An Jingang1,2(), Zhang Yi1,2, He Yang1,2
), An Jingang1,2(), Zhang Yi1,2, He Yang1,2
Received:2022-09-11
Revised:2022-12-27
Online:2023-02-01
Published:2023-02-21
Contact:
An Jingang
E-mail:kqfzq@hotmail.com;anjingang@126.com
CLC Number:
Feng Zhiqiang, An Jingang, Zhang Yi, He Yang. Surgical treatment of severe medication-related osteonecrosis of the jaw[J]. West China Journal of Stomatology, 2023, 41(1): 43-51.
Add to citation manager EndNote|Ris|BibTeX

Fig 1
Pre- and post-operative images of stage 2 MRONJ of the left mandible

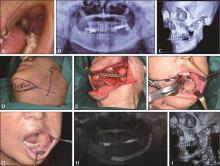
Fig 2
Pre- and post-operative images of stage 3 MRONJ of the left mandible
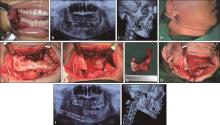
Fig 3
Pre- and post-operative images of stage 3 MRONJ of the right mandible

Fig 4
Pre- and post-operative images of stage 3 MRONJ of the right maxilla
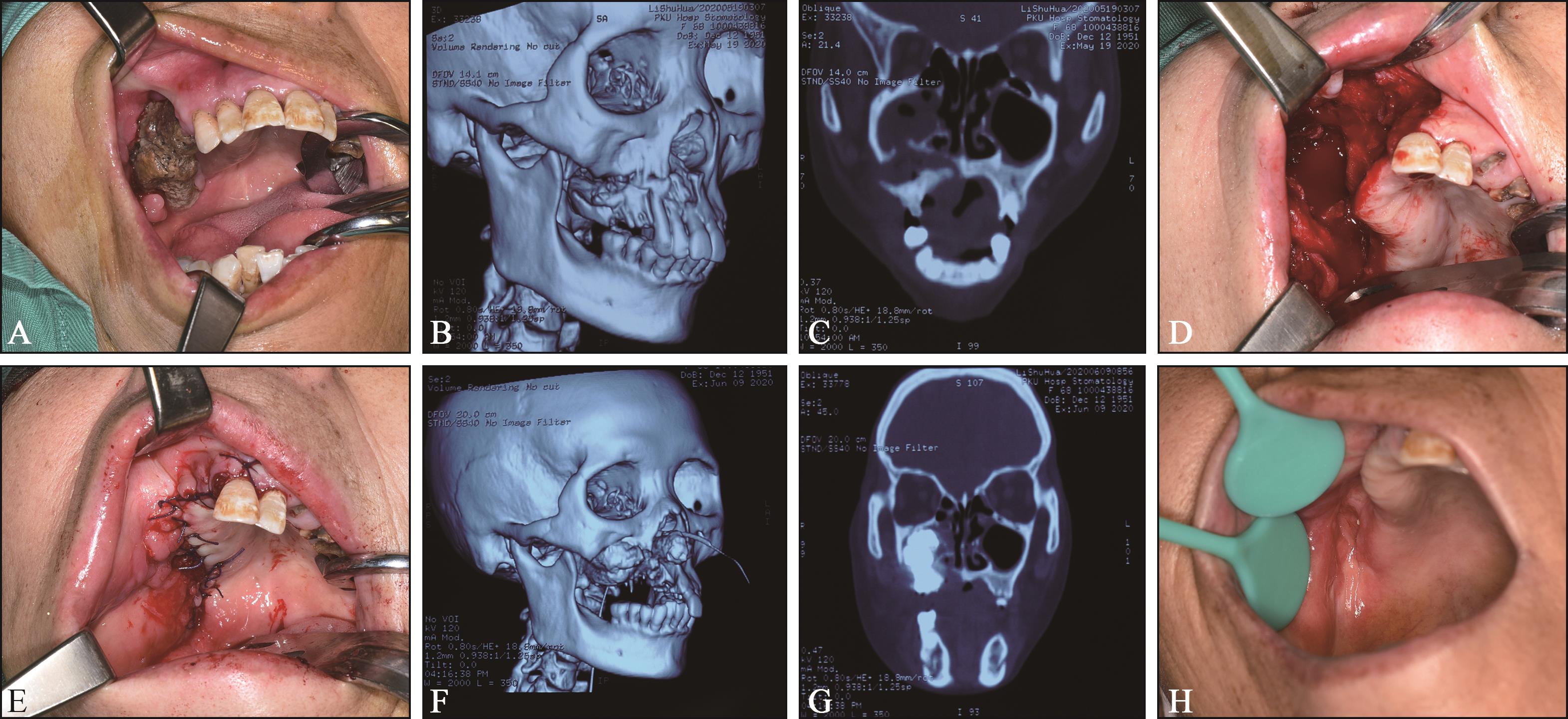
Fig 5
Pre- and post-operative images of stage 3 MRONJ of the right maxilla
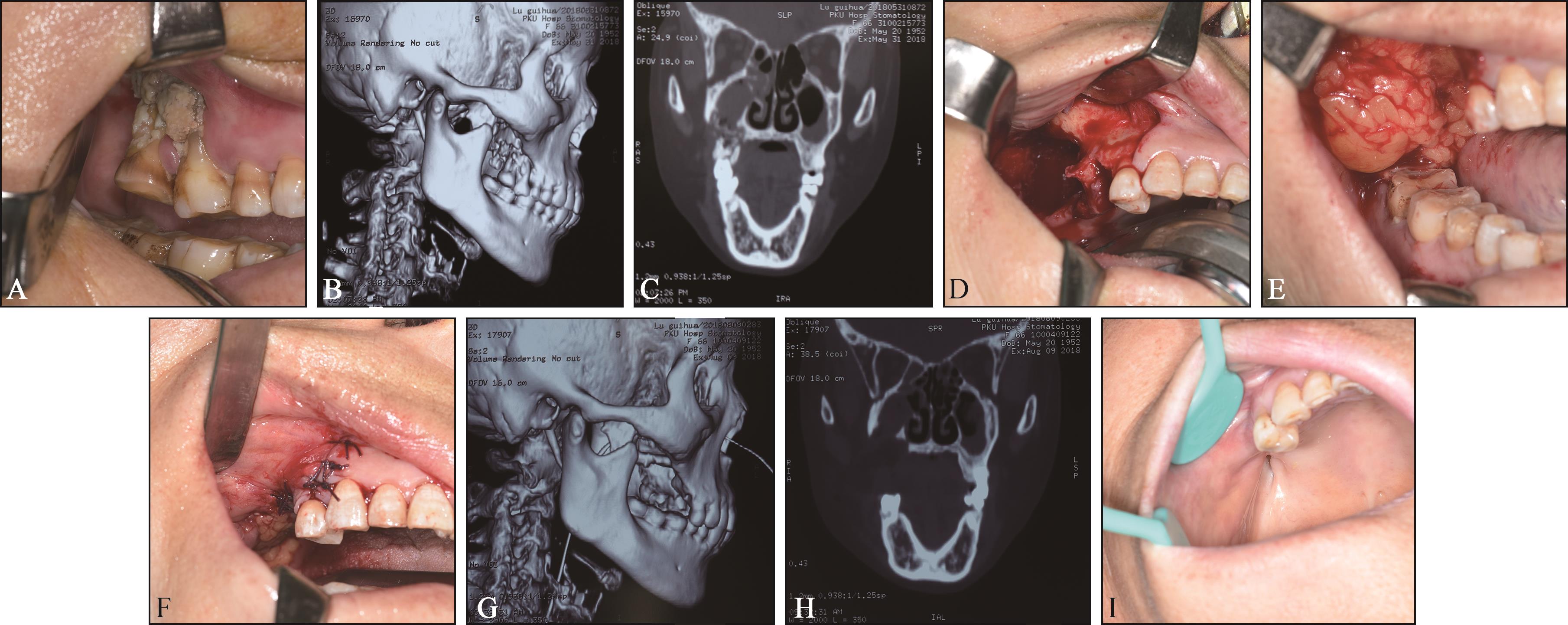

Fig 6
PRF adjuvant therapy for MRONJ
Tab 1
Clinical parameters of 104 patients with 123 sites of MRONJ
| 特征 | 数值 | |
|---|---|---|
| 性别 | 女性 | 62/59.6% |
| 男性 | 42/40.4% | |
| 年龄/岁 | 64.6±9.1 | |
| 原发疾病,恶性 | 91/87.5% | |
| 乳腺癌 | 31/29.8% | |
| 肺癌 | 24/23.1% | |
| 肾癌 | 12/11.5% | |
| 多发性骨髓瘤 | 10/9.6% | |
| 前列腺癌 | 8/7.7% | |
| 大肠癌 | 3/2.9% | |
| 软组织肉瘤 | 1/1.0% | |
| 阴道癌 | 1/1.0% | |
| 肝癌 | 1/1.0% | |
| 原发疾病,良性 | 13/12.5% | |
| 骨质疏松症 | 5/4.8% | |
| 类风湿性关节炎 | 5/4.8% | |
| 天疱疮 | 2/1.9% | |
| 朗格汉斯细胞增生症 | 1/1.0% | |
| 药物危险因素* | 唑来膦酸 | 89/85.6% |
| 阿仑膦酸钠 | 10/9.6% | |
| 帕米膦酸钠 | 10/9.6% | |
| 抗血管生成药物 | 62/59.6% | |
| BPs继以抗血管生成药物 | 59/56.7% | |
| 给药方式 | 静脉给药 | 93/89.4% |
| 口服给药 | 9/8.7% | |
| 口服+静脉给药 | 1/1.0% | |
| 皮下注射+静脉给药 | 1/1.0% | |
| BPs治疗时长/月 | 34.7±25.8 | |
| 停药时长/月 | 10.1±10.7 | |
| 发病潜伏期/月 | 33.9±25.3 | |
| 术前MRONJ持续时间/月 | 11.9±9.7 | |
| 糖尿病 | 22/21.2% | |
| 激素治疗 | 51/49.0% | |
| 化疗 | 61/58.7% | |
| 病变分期 | 2 | 43/35.0% |
| 3 | 80/65.0% | |
| 上下颌分布 | 上颌 | 39/31.7% |
| 下颌 | 84/68.3% | |
| 解剖部位 | 颌骨前部 (前牙区、前磨牙区) | 19/15.4% |
| 颌骨后部(磨牙区) | 104/84.6% | |
| 局部诱因 | 牙周/种植体周围疾病 | 95/77.2% |
| 拔牙/义齿创伤 | 22/17.9% | |
| 无明确诱因 | 6/4.9% |
| 1 | Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw-2014 update[J]. J Oral Maxillofac Surg, 2014, 72(10): 1938-1956. |
| 2 | Aljohani S, Troeltzsch M, Hafner S, et al. Surgical treatment of medication-related osteonecrosis of the upper jaw: case series[J]. Oral Dis, 2019, 25(2): 497-507. |
| 3 | Otto S, Pautke C, Van den Wyngaert T, et al. Medication-related osteonecrosis of the jaw: prevention, diagnosis and management in patients with cancer and bone metastases[J]. Cancer Treat Rev, 2018, 69: 177-187. |
| 4 | 安金刚, 吕晓鸣, 贾宽宽. 下颌下腺转位在下颌骨3期药物相关性颌骨坏死手术中的应用[J]. 中华口腔医学杂志, 2021, 56(5): 441-446. |
| An JG, Lü XM, Jia KK. Application of the submandibular gland for management of stage 3 medication-related osteonecrosis of the mandible[J]. Chin J Stomatol, 2021, 56(5): 441-446. | |
| 5 | Zhou W, Feng Z, An J, et al. Combined reconstruction plate fixation and submandibular gland translocation for the management of medication-related osteonecrosis of the mandible[J]. Int J Oral Maxillofac Surg, 2020, 49(12): 1584-1588. |
| 6 | 郭玉兴, 赵宁, 王佃灿, 等. 以带蒂颊脂垫为基础的双层软组织封闭技术修复药物相关颌骨坏死手术后上颌骨缺损的临床应用[J]. 华西口腔医学杂志, 2022, 40(1): 61-67. |
| Guo YX, Zhao N, Wang DC, et al. Clinical application of double-layer soft tissue closure technology based on pedicled buccal fat pad in repairing maxillary defects after medication-related osteonecrosis of jaw surgery[J]. West China J Stomatol, 2022, 40(1): 61-67. | |
| 7 | Nisi M, La Ferla F, Karapetsa D, et al. Conservative surgical management of patients with bisphosphonate-related osteonecrosis of the jaws: a series of 120 patients[J]. Br J Oral Maxillofac Surg, 2016, 54(8): 930-935. |
| 8 | Otto S, Ristow O, Pache C, et al. Fluorescence-guided surgery for the treatment of medication-related osteonecrosis of the jaw: a prospective cohort study[J]. J Craniomaxillofac Surg, 2016, 44(8): 1073-1080. |
| 9 | Favia G, Tempesta A, Limongelli L, et al. Medication-related osteonecrosis of the jaw: surgical or non-surgical treatment[J]. Oral Dis. 2018, 24(1/2): 238-242. |
| 10 | Ruggiero SL, Kohn N. Disease stage and mode of therapy are important determinants of treatment outcomes for medication-related osteonecrosis of the jaw[J]. J Oral Maxillofac Surg, 2015, 73(12 ): S94-S100. |
| 11 | Klingelhöffer C, Zeman F, Meier J, et al. Evaluation of surgical outcome and influencing risk factors in patients with medication-related osteonecrosis of the jaws[J]. J Craniomaxillofac Surg, 2016, 44(10): 1694-1699. |
| 12 | Hayashida S, Soutome S, Yanamoto S, et al. Evaluation of the treatment strategies for medication-related osteonecrosis of the jaws (MRONJ) and the factors affecting treatment outcome: a multicenter retrospective study wi-th propensity score matching analysis[J]. J Bone Miner Res, 2017, 32(10): 2022-2029. |
| 13 | El-Rabbany M, Sgro A, Lam DK, et al. Effectiveness of treatments for medication-related osteonecrosis of the jaw: a systematic review and meta-analysis[J]. J Am Dent Assoc, 2017, 148(8): 584-594.e2. |
| 14 | Kim HY, Lee SJ, Kim SM, et al. Extensive surgical procedures result in better treatment outcomes for bisphosphonate-related osteonecrosis of the jaw in patients with osteoporosis[J]. J Oral Maxillofac Surg, 2017, 75(7): 1404-1413. |
| 15 | Neto T, Horta R, Balhau R, et al. Resection and microvascular reconstruction of bisphosphonate-related osteonecrosis of the jaw: the role of microvascular reconstruction[J]. Head Neck, 2016, 38(8): 1278-1285. |
| 16 | Oteri G, De Ponte FS, Runci M, et al. Oral-health-rela-ted quality of life after surgical treatment of osteonecrosis of the jaws[J]. J Craniofac Surg, 2018, 29(2): 403-408. |
| 17 | Ristow O, Otto S, Troeltzsch M, et al. Treatment perspectives for medication-related osteonecrosis of the jaw (MRONJ)[J]. J Craniomaxillofac Surg, 2015, 43(2): 290-293. |
| 18 | Yoshiga D, Sasaguri M, Matsuo K, et al. Intraoperative detection of viable bone with fluorescence imaging u-sing visually enhanced lesion scope in patients with bisphosphonate-related osteonecrosis of the jaw: clinical and pathological evaluation[J]. Osteoporos Int, 2015, 26(7): 1997-2006. |
| 19 | Giovannacci I, Meleti M, Corradi D, et al. Clinical differences in autofluorescence between viable and nonvital bone: a case report with histopathologic evaluation performed on medication-related osteonecrosis of the jaws[J]. J Oral Maxillofac Surg, 2017, 75(6): 1216-1222. |
| 20 | Egyedi P. Utilization of the buccal fat pad for closure of oro-antral and/or oro-nasal communications[J]. J Oral Maxillofac Surg, 1977, 5(4): 241-244. |
| 21 | Hakobyan K, Poghosyan Y, Kasyan A. The use of buccal fat pad in surgical treatment of ‘Krokodil’ drug-relat-ed osteonecrosis of maxilla[J]. J Craniomaxillofac Surg, 2018, 46(5): 831-836. |
| 22 | Melville JC, Tursun R, Shum JW, et al. A technique for the treatment of oral-antral fistulas resulting from medication-related osteonecrosis of the maxilla: the combined buccal fat pad flap and radical sinusotomy[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2016, 122(3): 287-291. |
| 23 | Marx RE, Sawatari Y, Fortin M, et al. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment[J]. J Oral Maxillofac Surg, 2005, 63(11): 1567-1575. |
| 24 | Pautke C, Otto S, Reu S, et al. Bisphosphonate related osteonecrosis of the jaw-manifestation in a microvascular iliac bone flap[J]. Oral Oncol, 2011, 47(5): 425-429. |
| 25 | Pichardo SEC, Ten Broek FW, Richard van Merkesteyn JP. Treatment of pathologic fractures of the mandible in stage Ⅲ medication-related osteonecrosis of the jaw-an observational study[J]. J Craniomaxillofac Surg, 2018, 46(8): 1241-1246. |
| 26 | Troeltzsch M, Probst F, Troeltzsch M, et al. Conservative management of medication-related osteonecrosis of the maxilla with an obturator prosthesis[J]. J Prosthet Dent, 2015, 113(3): 236-241. |
| 27 | Mücke T, Jung M, Koerdt S, et al. Free flap reconstruction for patients with bisphosphonate related osteonecrosis of the jaws after mandibulectomy[J]. J Craniomaxillofac Surg, 2016, 44(2): 142-147. |
| 28 | Caldroney S, Ghazali N, Dyalram D, et al. Surgical resection and vascularized bone reconstruction in advanced stage medication-related osteonecrosis of the jaw[J]. Int J Oral Maxillofac Surg, 2017, 46(7): 871-876. |
| 29 | Nisi M, La Ferla F, Karapetsa D, et al. Risk factors influencing BRONJ staging in patients receiving intravenous bisphosphonates: a multivariate analysis[J]. Int J Oral Maxillofac Surg, 2015, 44(5): 586-591. |
| 30 | Kwon YD, Kim DY, Ohe JY, et al. Correlation between serum C-terminal cross-linking telopeptide of typeⅠcollagen and staging of oral bisphosphonate-related osteonecrosis of the jaws[J]. J Oral Maxillofac Surg, 2009, 67(12): 2644-2648. |
| 31 | Bagan JV, Jimenez Y, Gomez D, et al. Collagen telopeptide (serum CTX) and its relationship with the size and number of lesions in osteonecrosis of the jaws in cancer patients on intravenous bisphosphonates[J]. Oral Oncol, 2008, 44(11): 1088-1089. |
| 32 | Lorenzo-Pouso AI, Pérez-Sayáns M, González-Palanca S, et al. Biomarkers to predict the onset of biphosphonate-related osteonecrosis of the jaw: a systematic review[J]. Med Oral Patol Oral Cir Bucal, 2019, 24(1): e26-e36. |
| 33 | Bagan L, Jimenez Y, Leopoldo M, et al. Serum levels of RANKL and OPG, and the RANKL/OPG ratio in bis-phosphonate-related osteonecrosis of the jaw: are they useful biomarkers for the advanced stages of osteonecrosis[J]. Med Oral Patol Oral Cir Bucal, 2017, 22(5): e542-e547. |
| 34 | Feng Z, An J, Zhang Y. Factors influencing severity of medication-related osteonecrosis of the jaw: a retrospective study[J]. J Oral Maxillofac Surg, 2021, 79(8): 1683-1688. |
| [1] | Wu Min, Yin Heng, Chen Lixian, Shi Bing, Li Yang.. Analysis of risk factors affecting poor wound healing after primary cleft palate surgery [J]. West China Journal of Stomatology, 2023, 41(6): 719-724. |
| [2] | Han Yue, Liu Yixuan, Zhao Jihong, Zhong Haoyan. Cemento-ossifying fibroma resection combined with heterotopic canine autotransplantation: a case report [J]. West China Journal of Stomatology, 2023, 41(6): 731-736. |
| [3] | Wang Xudong, Wei Hongpu, Li Biao.. From “Empirical Surgery” to “Precision Surgery”: establishment and clinical application of precision orthognathic surgery system [J]. West China Journal of Stomatology, 2023, 41(5): 491-501. |
| [4] | Luo En.. Treatment of dentofacial deformities secondary to condylar hyperplasia [J]. West China Journal of Stomatology, 2023, 41(4): 369-376. |
| [5] | Hu Nan, Liu Chunxu, Gao Jing, Xie Chenyang, Yu Jiayi, Jia Luming, Yu Haiyang.. Simultaneous implantation and tooth preparation technology guided by 3D-printed guide [J]. West China Journal of Stomatology, 2023, 41(4): 483-490. |
| [6] | Huang Jiayue, Liu Xian, Wang Yan, Bao Chongyun.. Effect of dental follicles in minimally invasive open-eruption technique of labially impacted maxillary central incisors [J]. West China Journal of Stomatology, 2023, 41(2): 197-202. |
| [7] | Song Dongzhe, Luo Yu, Liu Xian, Hu Pei, Huang Dingming. Combined micro-apical surgery and vital pulp therapy in mandibular second molars with external root resorption caused by impacted teeth [J]. West China Journal of Stomatology, 2023, 41(2): 225-231. |
| [8] | Lin Chengzhong, Zhang Yong, Dong Shao, Wu Jinyang, Zhang Chuxi, Wan Xinjun, Zhang Shilei. Application of mixed reality-based surgical navigation system in craniomaxillofacial trauma bone reconstruction [J]. West China Journal of Stomatology, 2022, 40(6): 676-684. |
| [9] | Zhu Songsong, Wang Xudong, Yang Xuewen, Wang Xiaoxia, Tian Lei, Liu Shuguang, Zheng Guangsen, Tang Zhenglong, Wu Guomin, Li Zhiyong, Bai Xiaofeng, Huang Xuanping, Huang Li, Xi Weihong, Zhu Yaomin. Experts’ consensus on precaution and treatment for complications of sagittal split ramus osteotomy [J]. West China Journal of Stomatology, 2022, 40(3): 247-254. |
| [10] | Li Chunjie, Han Bo, Zhu Guiquan.. Vessel anastomosis in free flap reconstruction for oral and maxillofacial defects: techniques and key points [J]. West China Journal of Stomatology, 2022, 40(3): 271-278. |
| [11] | Kang Zebiao, Mai Xiaoxue, Wang Xin, Xie Fuqiang. Evaluation of the postoperative effect of computer-assisted free fibula mandibular reconstruction [J]. West China Journal of Stomatology, 2022, 40(2): 189-196. |
| [12] | Jiang Yueyun, Tang Lingling, Ma Zhongkai, Liu Wei, Huang Nengwen, Li Chunjie. Application of vascularized mucosal flap for early-medium-term tongue cancer and floor of mouth cancer defect repair: a preliminary study [J]. West China Journal of Stomatology, 2022, 40(2): 204-209. |
| [13] | Guo Yuxing, Zhao Ning, Wang Diancan, Wang Yang, Guo Chuanbin. Clinical application of double-layer soft tissue closure technology based on pedicled buccal fat pad in repairing maxillary defects after medication-related osteonecrosis of jaw surgery [J]. West China Journal of Stomatology, 2022, 40(1): 61-67. |
| [14] | Yin Yin, Zeng Wei, Jing Wei, Tang Wei, Guo Weihua. Evaluation of hyperbaric oxygen therapy for the osteoradionecrosis of the jaws: Meta-analysis [J]. West China Journal of Stomatology, 2021, 39(6): 690-697. |
| [15] | Zhao Ning, Liu Zhenguo, Xu Yaoxiang, Yue Jin, Xue Lingfa, Xiao Wenlin. Clinical study on obstructive sleep apnea following pharyngeal flap surgery [J]. West China Journal of Stomatology, 2021, 39(5): 566-569. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 This work is licensed under a Creative Commons Attribution 3.0 License.
This work is licensed under a Creative Commons Attribution 3.0 License.
