| 1 |
Japanese Allied Committee on Osteonecrosis of the Jaw, Yoneda T, Hagino H, et al. Antiresorptive agent-related osteonecrosis of the jaw: position paper 2017 of the Japanese allied committee on osteonecrosis of the jaw[J]. J Bone Miner Metab, 2017, 35(1): 6-19.
|
| 2 |
Hayashida S, Soutome S, Yanamoto S, et al. Evaluation of the treatment strategies for medication-related osteonecrosis of the jaws (MRONJ) and the factors affecting treatment outcome: a multicenter retrospective study wi-th propensity score matching analysis[J]. J Bone Miner Res, 2017, 32(10): 2022-2029.
|
| 3 |
Guo Y, Guo C. Enhancement of bone perfusion through cortical perforations to improve healing of medication-related osteonecrosis of the jaw: a retrospective study[J]. Int J Oral Maxillofac Surg, 2021, 50(6): 740-745.
|
| 4 |
Ruggiero SL, Dodson TB, Fantasia J, et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw: 2014 update[J]. J Oral Maxillofac Surg, 2014, 72(10): 1938-1956.
|
| 5 |
郭玉兴, 王佃灿, 王洋, 等. 二膦酸盐药物治疗乳腺癌骨转移发生颌骨坏死的临床特点[J]. 北京大学学报(医学版), 2016, 48(1): 80-83.
|
|
Guo YX, Wang DC, Wang Y, et al. Clinical features of osteonecrosis of jaws after bisphosphonates therapy for bone metastasis of breast cancer[J]. J Peking Univ (He-alth Sci), 2016, 48(1): 80-83.
|
| 6 |
Fusco V, Porta C, Saia G, et al. Osteonecrosis of the jaw in patients with metastatic renal cell cancer treated with bisphosphonates and targeted agents: results of an Italian multicenter study and review of the literature[J]. Clin Genitourin Cancer, 2015, 13(4): 287-294.
|
| 7 |
Khan AA, Morrison A, Hanley DA, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus[J]. J Bone Miner Res, 2015, 30(1): 3-23.
|
| 8 |
Li QX, Pu YF, Lu H, et al. Porphyromonas, Treponema, and Mogibacterium promote IL8/IFNγ/TNFα-based pro-inflammation in patients with medication-related osteonecrosis of the jaw[J]. J Oral Microbiol, 2020, 13(1): 1851112.
|
| 9 |
Di Fede O, Panzarella V, Mauceri R, et al. The dental management of patients at risk of medication-related osteonecrosis of the jaw: new paradigm of primary prevention[J]. Biomed Res Int, 2018, 2018: 2684924.
|
| 10 |
Owosho AA, Liang STY, Sax AZ, et al. Medication-related osteonecrosis of the jaw: an update on the memorial Sloan Kettering cancer center experience and the role of premedication dental evaluation in prevention[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2018, 125(5): 440-445.
|
| 11 |
Kim T, Kim S, Song MJ, et al. Removal of pre-existing periodontal inflammatory condition before tooth extraction ameliorates medication-related osteonecrosis of the jaw-like lesion in mice[J]. Am J Pathol, 2018, 188(10): 2318-2327.
|
| 12 |
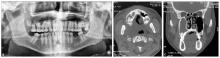
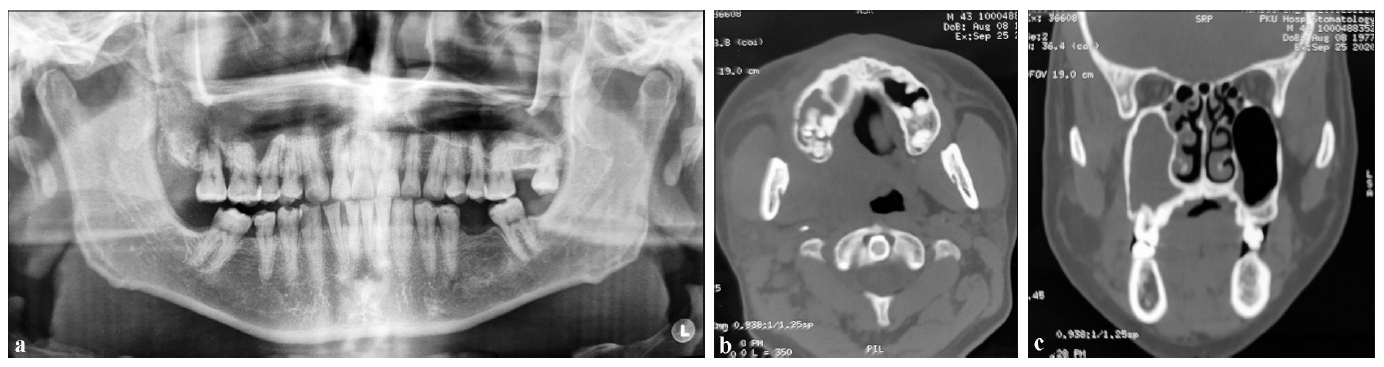
Guo YX, Wang DC, Wang Y, et al. Imaging features of medicine-related osteonecrosis of the jaws: comparison between panoramic radiography and computed tomography[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2016, 122(2): e69-e76.
|
| 13 |
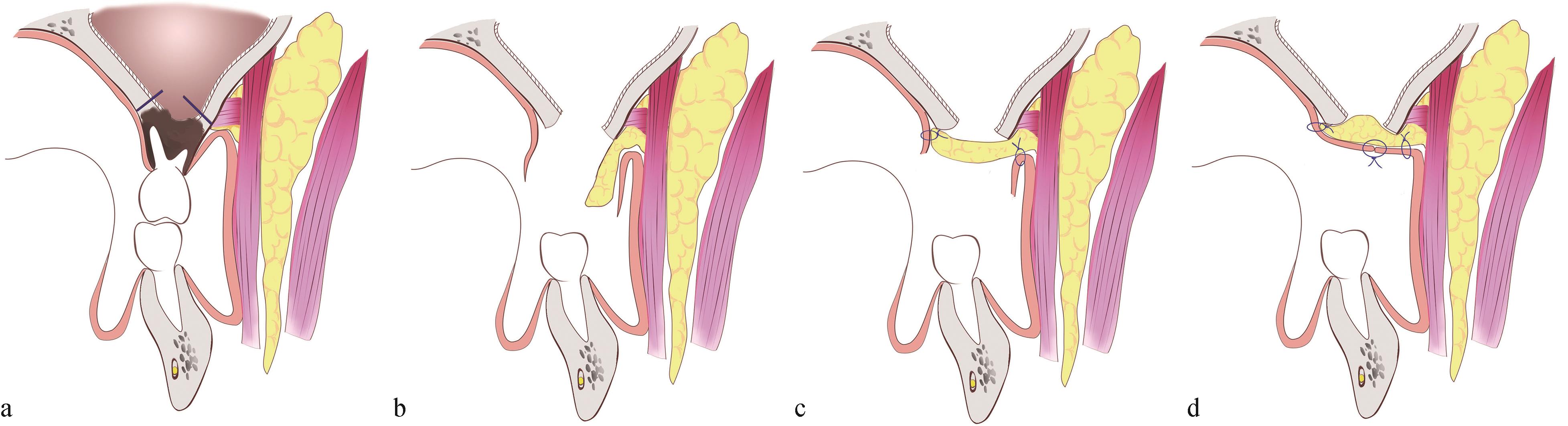
Ristow O, Ruckschloss T, Bodem J, et al. Double-layer closure techniques after bone surgery of medication-related osteonecrosis of the jaw—a single center cohort study[J]. J Craniomaxillofac Surg, 2018, 46(5): 815-824.
|

 ), Zhao Ning1,2, Wang Diancan1,2, Wang Yang1,2, Guo Chuanbin1,2(
), Zhao Ning1,2, Wang Diancan1,2, Wang Yang1,2, Guo Chuanbin1,2( This work is licensed under a Creative Commons Attribution 3.0 License.
This work is licensed under a Creative Commons Attribution 3.0 License.